Histological Architecture of Gastric Epithelial Neoplasias That Showed Absent Microsurface Patterns, Visualized by Magnifying Endoscopy with Narrow-Band Imaging
- Chuman K
 1,2
1,2 - Yao K1
- Kanemitsu T1
- Nagahama T1
- Miyaoka M1
- Takahashi H2
- Imamura K3
- Hasegawa R1
- Ueki T3
- Tanabe H3
- Haraoka S2
- Iwashita A2
- Affiliations
-
- 1Department of Endoscopy, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- 2Department of Pathology, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- 3Department of Gastroenterology, Fukuoka University Chikushi Hospital, Fukuoka, Japan
- KMID: 2514176
- DOI: http://doi.org/10.5946/ce.2020.090
Abstract
- Background/Aims
The objective of this study was to elucidate the histological structure of the absent microsurface patterns (MSPs) that were visualized by magnifying endoscopy with narrow-band imaging (M-NBI).
Methods
The study included consecutive gastric epithelial neoplasias for which M-NBI findings and histological findings could be compared on a one-to-one basis. The lesions were classified as absent MSPs and present MSPs based on the findings obtained using M-NBI. Of the histopathological findings for each lesion that corresponded to M-NBI findings, crypt opening densities, crypt lengths, crypt opening diameters, intercrypt distances, and crypt angles were measured and compared.
Results
Thirty-six lesions were included in the analysis; of these, 17 lesions exhibited absent MSP and 19 lesions exhibited present MSP. Comparing the histological measurements for absent MSPs vs. present MSPs, median crypt opening density was 0.9 crypt openings/mm vs. 4.8 crypt openings/mm (p<0.001), respectively. The median crypt length, median crypt opening diameter, median intercrypt distance, and median crypt angle were 80.0 μm vs. 160 μm (p<0.001), 40.0 μm vs. 44.2 μm (p=0.09), 572.5 μm vs. 166.7 μm (p<0.001), and 21.6 degrees vs. 15.5 degrees (p<0.001), respectively.
Conclusions
Histological findings showed that lesions exhibiting absent MSPs had lower crypt opening density, shorter crypt length, greater intercrypt distance, and larger crypt angle.
Figure
-
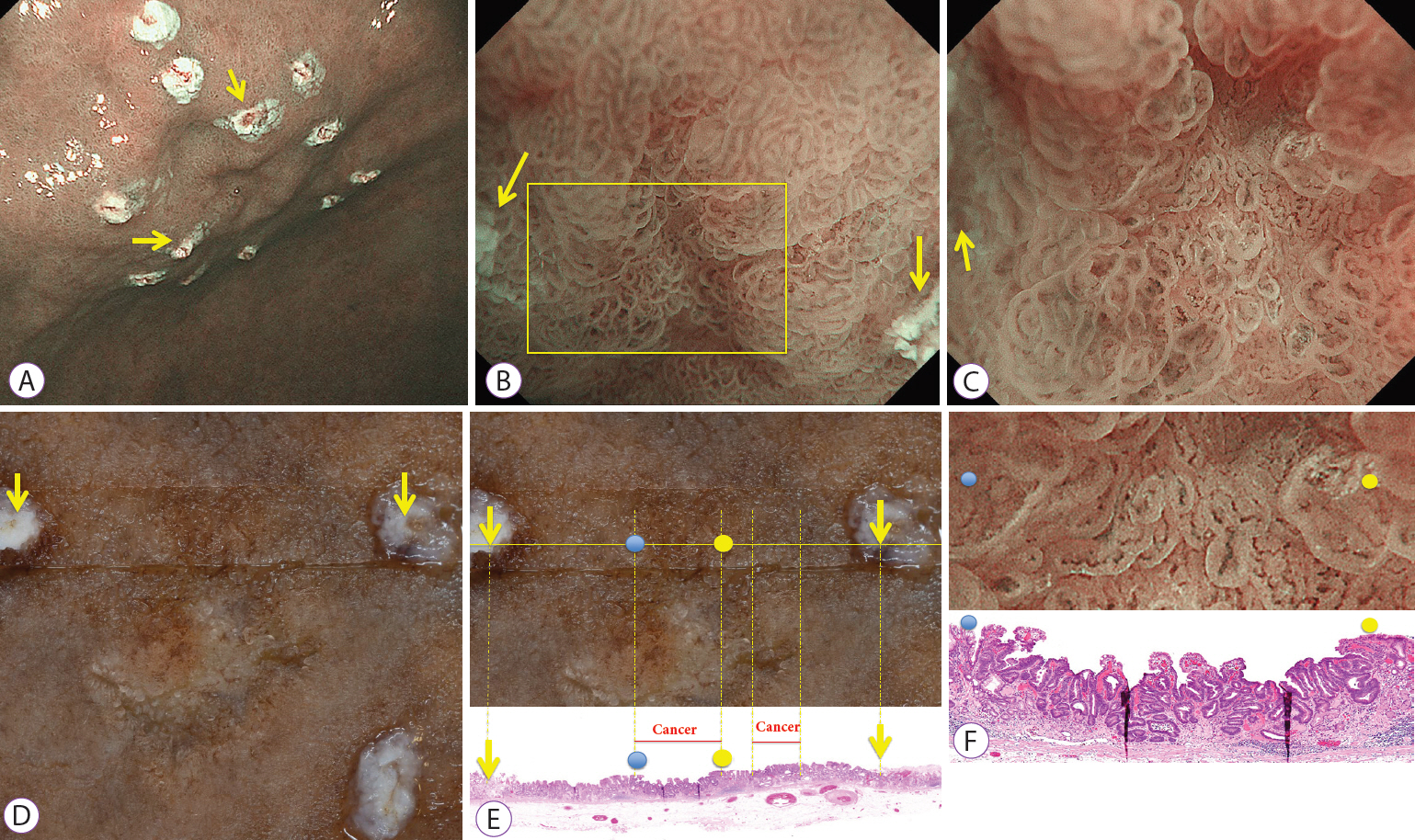
Fig. 1. Correspondence between the regions of interest in images obtained by magnifying endoscopy with narrow-band imaging (M-NBI) and matching histological findings. (A) Image obtained by M-NBI. In addition to marks added before endoscopic submucosal dissection (ESD) to indicate the extent of the resection, M-NBI was used to place marks at two points on either side of the lesion. (B) M-NBI: weak magnification. Magnified observation of the area between the two marks was performed by M-NBI (the arrows indicate the marks). (C) M-NBI: maximum magnification. Magnified observation was performed for the area enclosed by the square shown in (B), and the recorded endoscopic findings were used (arrows indicate marks). (D) Formalin-fixed specimen after ESD. After the lesion was resected by ESD, stretched, and fixed in place on a rubber plate with pins, the two marks made before ESD were identified. A cut was made between the two marks, sections were prepared, and hematoxylin-eosin staining was performed. (E) Post-ESD formalin-fixed specimens (top) matched with histological findings (bottom). Marks on the prepared sections were first identified, and histological findings for the area between the marks were observed (arrows indicate marks). Blue and yellow circles on the resected specimen at the top correspond, respectively, to the blue and yellow circles in the histological findings on the bottom. (F) Correspondence between M-NBI (maximum magnification, top) and histological findings (bottom). Histological findings corresponding to the region of interest in the image obtained by M-NBI were identified using the two marks from before the resection (C) and the two marks in the histological findings (E). Blue and yellow circles on the image obtained by M-NBI at the top correspond, respectively, to the blue and yellow circles in the histological findings on the bottom.
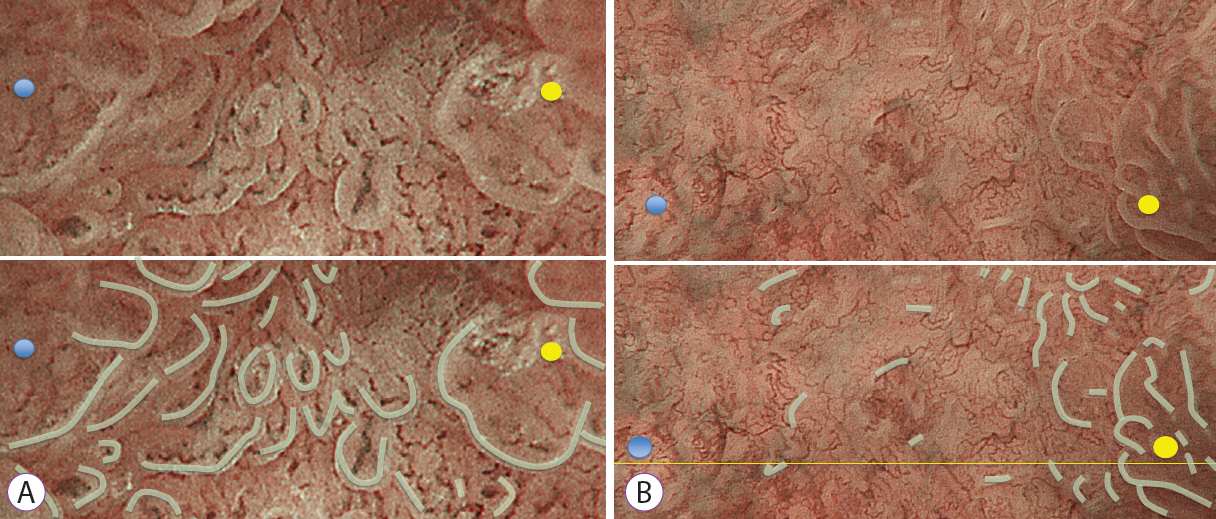
Fig. 2. Assessment of microsurface patterns (MSPs). (A) Present MSPs (bottom: marginal crypt epithelium traced with gray line). (B) Absent MSPs (bottom: marginal crypt epithelium traced with gray line).
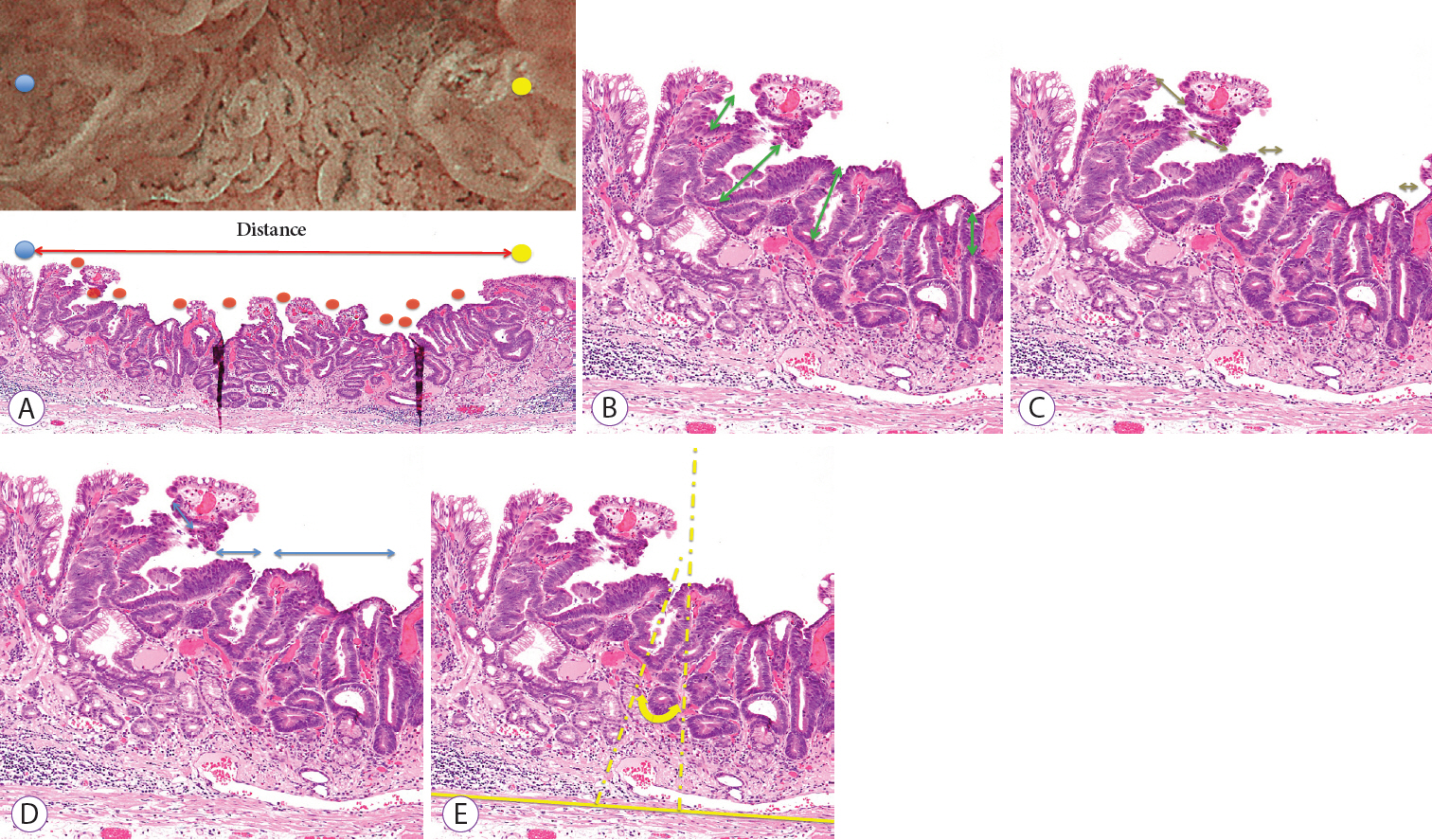
Fig. 3. Histological measurements. (A) Crypt openings density = number of crypt openings / examined distance. The red circles indicate crypt openings. (B) Crypt length (double-headed arrow). (C) Crypt opening diameter (double-headed arrow). (D) Intercrypt distance (double-headed arrow). (E) Crypt angle (double-headed arrow).
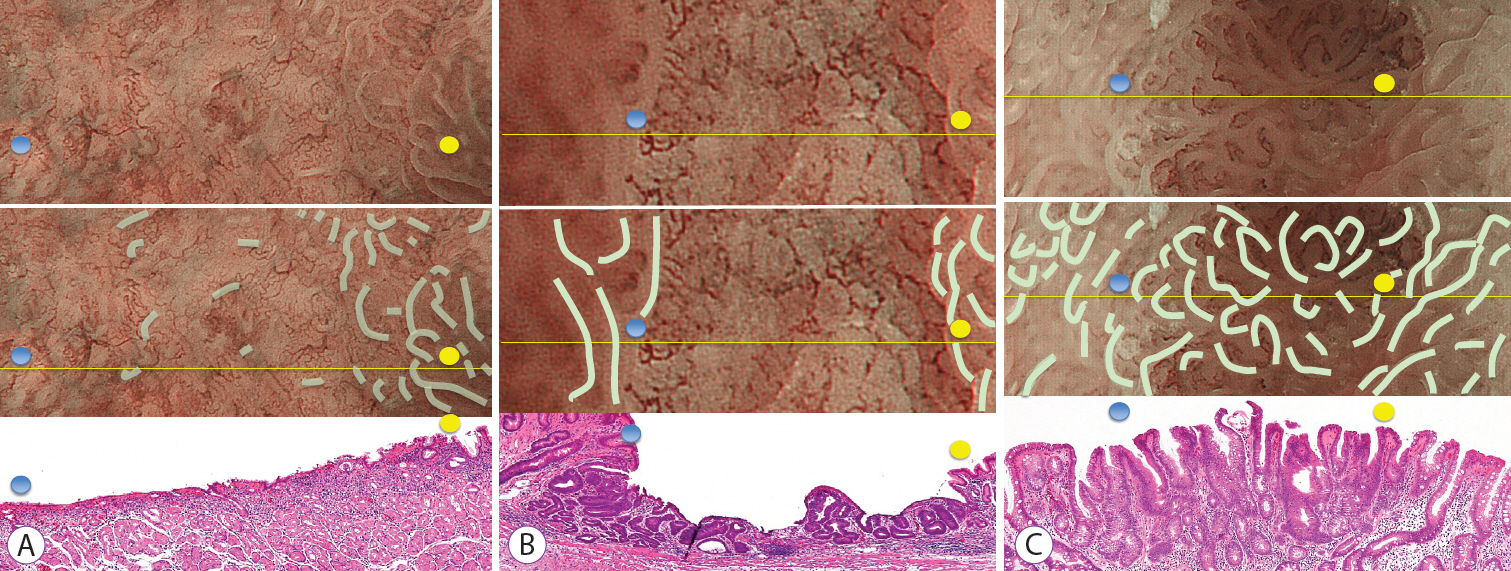
Fig. 4. Typical examples and histological measurements (mean±standard deviation for crypt length, crypt opening diameter, intercrypt distance, and crypt angle) for the absent microsurface pattern (MSP) and present MSP groups. (A) Example of early gastric cancer showing an absent MSP using magnifying endoscopy with narrow-band imaging (M-NBI). Histological findings indicated moderately to poorly differentiated adenocarcinomas. It’s crypt opening density was 2 crypt openings/mm, crypt length was 80±87.5 μm, crypt opening diameter was 35.0±8.7 μm, intercrypt distance was 256.7±140.1 μm, and crypt angle was 15.5±20.9 degrees. (B) Example of early gastric cancer showing an absent MSP using M-NBI. Histological findings showed a well-differentiated adenocarcinoma. It’s crypt opening density was 1.71 crypt openings/mm, crypt length was 100±25 μm, crypt opening diameter was 56.7±5.8 μm, intercrypt distance was 350±282.3 μm, and crypt angle was 27.3±19.6 degrees. (C) Example of early gastric cancer showing a present MSP. Histological findings demonstrated a well-differentiated adenocarcinoma. It’s crypt opening density was 6.28 crypt openings/mm, crypt length was 224.5±101.3 μm, crypt opening diameter was 40.9±18.7 μm, intercrypt distance was 120±48.5 μm, and crypt angle was 12.5±12.5 degrees.
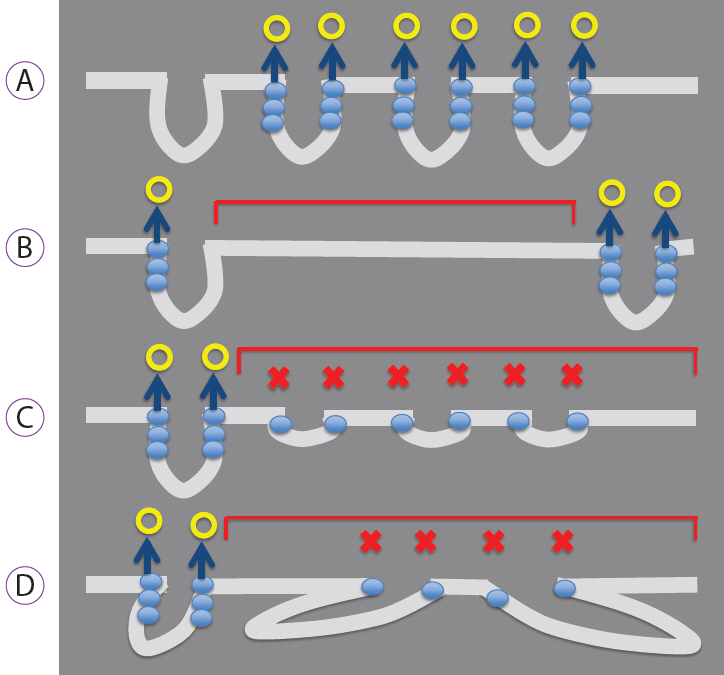
Fig. 5. Mechanisms by which the marginal crypt epithelium is visualized and not visualized. (A) Mechanism of visualization. Backward scattering caused by the marginal crypt epithelium (blue circle) is vertically integrated (blue arrow), and the epithelium is visualized (yellow circle). (B-D) Mechanisms that make visualization difficult. (B) If the crypt opening density is low or the intercrypt distance large, the number of crypts that cause backward scattering (blue circle) is reduced, resulting in the absent microsurface pattern (MSP; red square brackets). (C) If the crypt length is short or (D) the crypt angle is large (i.e., crypts run obliquely), the backward scatter (blue circle) does not integrate vertically. Consequently, the epithelium is not visualized as a white, belt-like structure (marginal crypt epithelium), resulting in the absent MSP (red square brackets).
Reference
-
1. Ezoe Y, Muto M, Uedo N, et al. Magnifying narrowband imaging is more accurate than conventional white-light imaging in diagnosis of gastric mucosal cancer. Gastroenterology. 2011; 141:2017–2025.e3.
Article2. Uedo N, Ishihara R, Iishi H, et al. A new method of diagnosing gastric intestinal metaplasia: narrow-band imaging with magnifying endoscopy. Endoscopy. 2006; 38:819–824.
Article3. Kanemitsu T, Yao K, Nagahama T, et al. The vessels within epithelial circle (VEC) pattern as visualized by magnifying endoscopy with narrow-band imaging (ME-NBI) is a useful marker for the diagnosis of papillary adenocarcinoma: a case-controlled study. Gastric Cancer. 2014; 17:469–477.
Article4. Kanesaka T, Sekikawa A, Tsumura T, et al. Absent microsurface pattern is characteristic of early gastric cancer of undifferentiated type: magnifying endoscopy with narrow-band imaging. Gastrointest Endosc. 2014; 80:1194–1198.e1.
Article5. Kanesaka T, Sekikawa A, Tsumura T, et al. Dense-type crypt opening seen on magnifying endoscopy with narrow-band imaging is a feature of gastric adenoma. Dig Endosc. 2014; 26:57–62.
Article6. Nakayoshi T, Tajiri H, Matsuda K, Kaise M, Ikegami M, Sasaki H. Magnifying endoscopy combined with narrow band imaging system for early gastric cancer: correlation of vascular pattern with histopathology (including video). Endoscopy. 2004; 36:1080–1084.
Article7. Doyama H, Yoshida N, Tsuyama S, et al. The “white globe appearance” (WGA): a novel marker for a correct diagnosis of early gastric cancer by magnifying endoscopy with narrow-band imaging (M-NBI). Endosc Int Open. 2015; 3:E120–E124.
Article8. Yagi K, Nozawa Y, Endou S, Nakamura A. Diagnosis of early gastric cancer by magnifying endoscopy with NBI from viewpoint of histological imaging: mucosal patterning in terms of white zone visibility and its relationship to histology. Diagn Ther Endosc. 2012; 2012:954809.
Article9. Kobayashi M, Takeuchi M, Ajioka Y, et al. Mucin phenotype and narrow-band imaging with magnifying endoscopy for differentiated-type mucosal gastric cancer. J Gastroenterol. 2011; 46:1064–1070.
Article10. Uchita K, Yao K, Uedo N, et al. Highest power magnification with narrow-band imaging is useful for improving diagnostic performance for endoscopic delineation of early gastric cancers. BMC Gastroenterol. 2015; 15:155.
Article11. Yao K, Imamura K, Yamaoka R, et al. [How to construct for gastrointrestinal imaging]. Stomach and Intestine. 2016; 51:1131–1148.12. Doyama H, Nakanishi H, Yoshida N, Takeda Y, Tsuyama S, Kurumaya H. [Techniques for comparing endoscopic and histopathological results in early gastric cancer]. Stomach and Intestine. 2016; 51:1203–1210.13. Yao K, Anagnostopoulos GK, Ragunath K. Magnifying endoscopy for diagnosing and delineating early gastric cancer. Endoscopy. 2009; 41:462–467.
Article14. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011; 14:101–112.15. Yao K. Zoom gastroscopy: magnifying endoscopy in the stomach. Tokyo: Springer Japan;2014.16. Yagi K, Saka A, Nozawa Y, Nakamura A, Umezu H. [The characteristic finding of histological mixed type of gastric adenocarcinoma in magnifying endoscopy]. Stomach and Intestine. 2013; 48:1609–1618.17. Phalanusitthepha C, Grimes KL, Ikeda H, et al. Endoscopic features of early-stage signet-ring-cell carcinoma of the stomach. World J Gastrointest Endosc. 2015; 7:741–746.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Role of Magnifying Endoscopy with Narrow-band Imaging in the Diagnosis of Early Gastric Cancer
- Usefulness of Narrow-Band Imaging in Endoscopic Submucosal Dissection of the Stomach
- Application of artificial intelligence for diagnosis of early gastric cancer based on magnifying endoscopy with narrow-band imaging
- Image-Enhanced Endoscopy and Its Corresponding Histopathology in the Stomach
- What Have We Accomplished in Endoscopic Image Analysis for Atrophic Gastritis?
