Secondary Neurulation Defects-1 : Retained Medullary Cord
- Affiliations
-
- 1Division of Pediatric Neurosurgery, Seoul National University Children's Hospital, Seoul, Korea
- 2Department of Anatomy, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2501717
- DOI: http://doi.org/10.3340/jkns.2020.0052
Abstract
- Retained medullary cord (RMC) is a relatively recent term. Pang et al. newly defined the RMC as a late arrest of secondary neurulation leaving a non-functional vestigial portion at the tip of the conus medullaris. RMC, which belongs to the category of closed spinal dysraphism, is a cord-like structure that is elongated from the conus toward the cul-de-sac. Because intraoperative electrophysiological confirmation of a non-functional conus is essential for the diagnosis of RMC, only a tentative or an assumptive diagnosis is possible before surgery or in cases of limited surgical exposure. We suggest the term ‘possible RMC’ for these cases. An RMC may cause tethered cord syndrome and thus requires surgery. This article reviews the literature to elucidate the pathoembryogenesis, clinical significance and treatment of RMCs.
Keyword
Figure
-
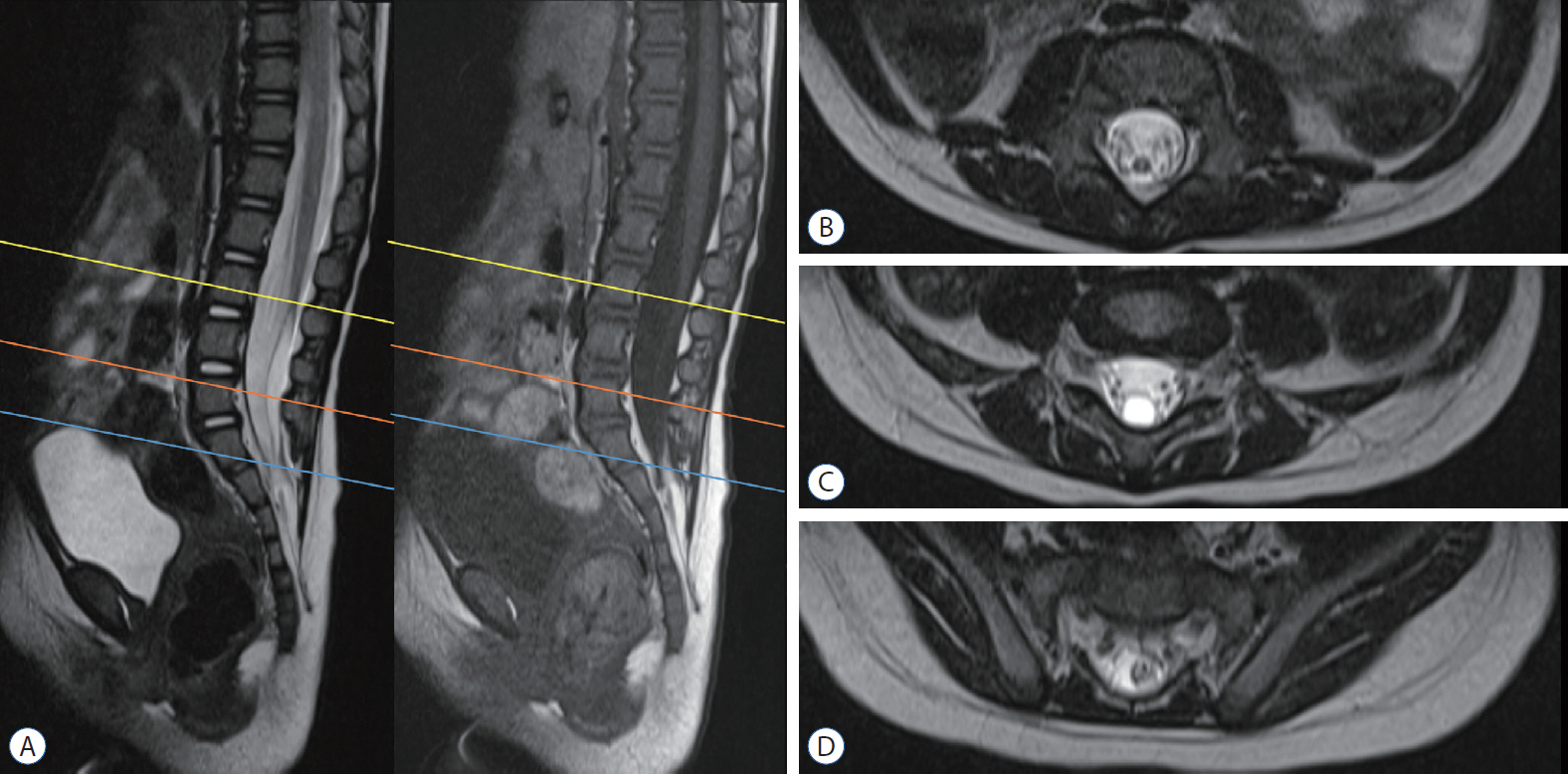
Fig. 1. Magnetic resonance imaging of a patient with ‘terminal syrinx with low-lying conus’. a : This demonstrates that the thick medullary cord extends down to the lower lumbar area, where it ends with a cyst that attaches to the cul-de-sac. B-D : They show T2 axial images at L3 (yellow line in a), L5 (orange line), and S1–2 (blue line), respectively.
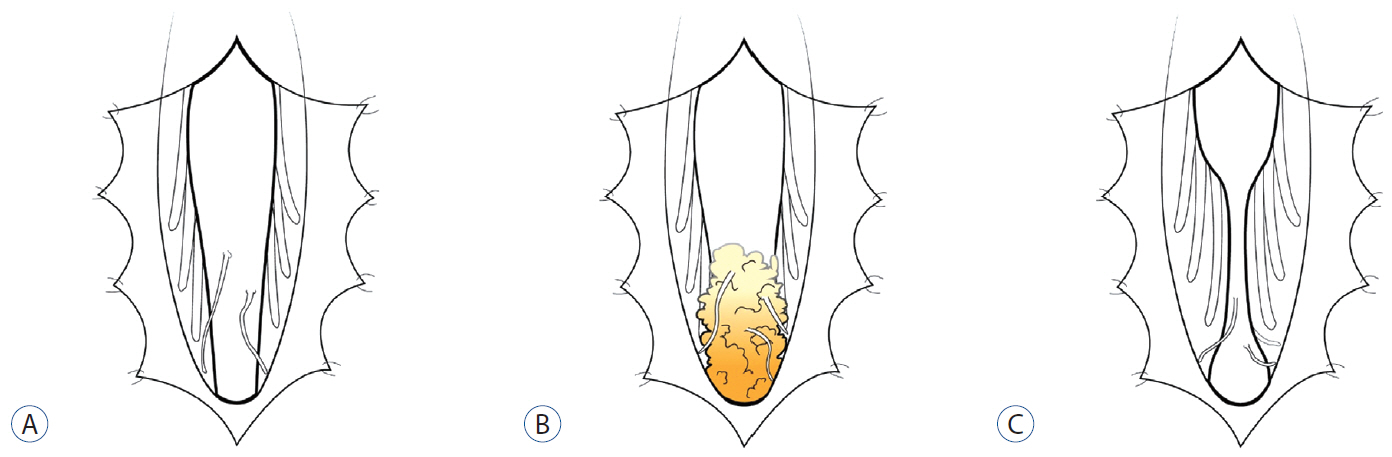
Fig. 2. Schematic illustrations of three types of non-cystic RMCs. Fine vestigial nerve twigs emanate from the medullary cord. a : It shows a typical RMC. B : It reveals no terminal tapering but enlargement of the conus with gradual transition to a fat-containing mass at the end. The ‘cord portion’ has a non-functional part in the RMC, which is different from a simple caudal lipoma. C : It shows an hourglass-shaped RMC with an intervening filum-like structure between the conus and RMC. If the part distal to the filum-like structure is functional but not electrophysiologically connected to the ‘upper cord’, it is considered a junctional neural tube defect. RMC : retained medullary cord.
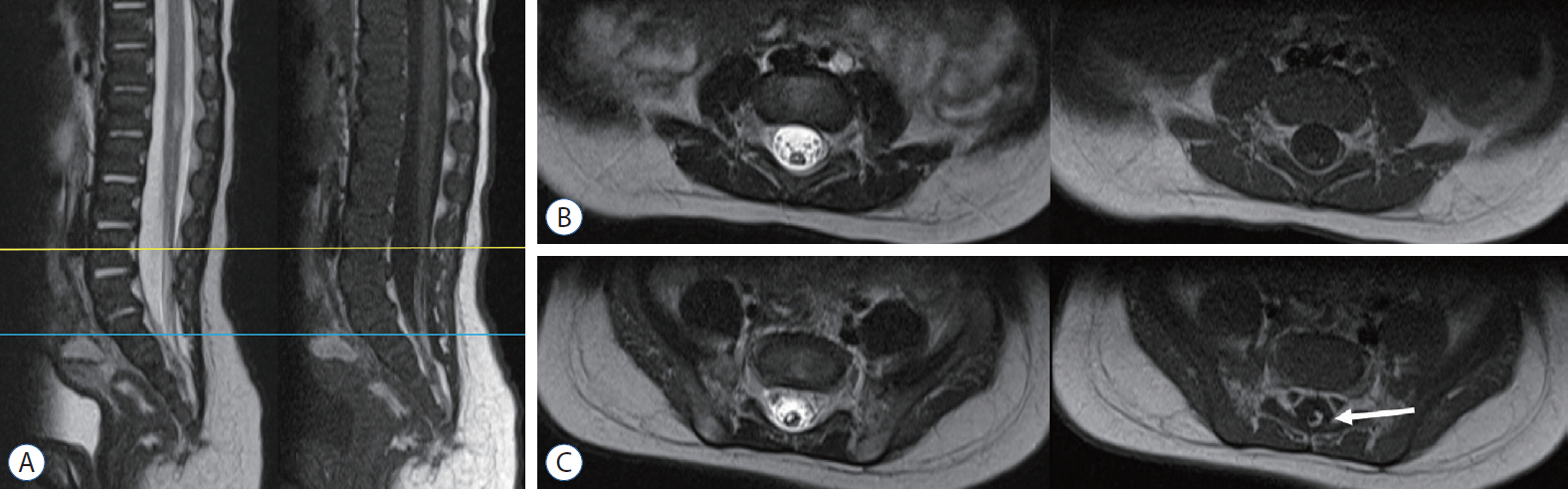
Fig. 3. MRI of a ‘possible retained medullary cord’ patient. a : The medullary cord partially contains fat tissue, resulting in high signal intensity in the T1-weighted MR image (arrow in C). In this case, only a small segment of the distal part was resected through a limited exposure of the lipoma. Exploration of the whole conus area, which may include the non-functional parts, was not performed. B and C : They show axial images at L4 (yellow line in a) and S1 (blue line), respectively. MRI : magnetic resonance imaging.
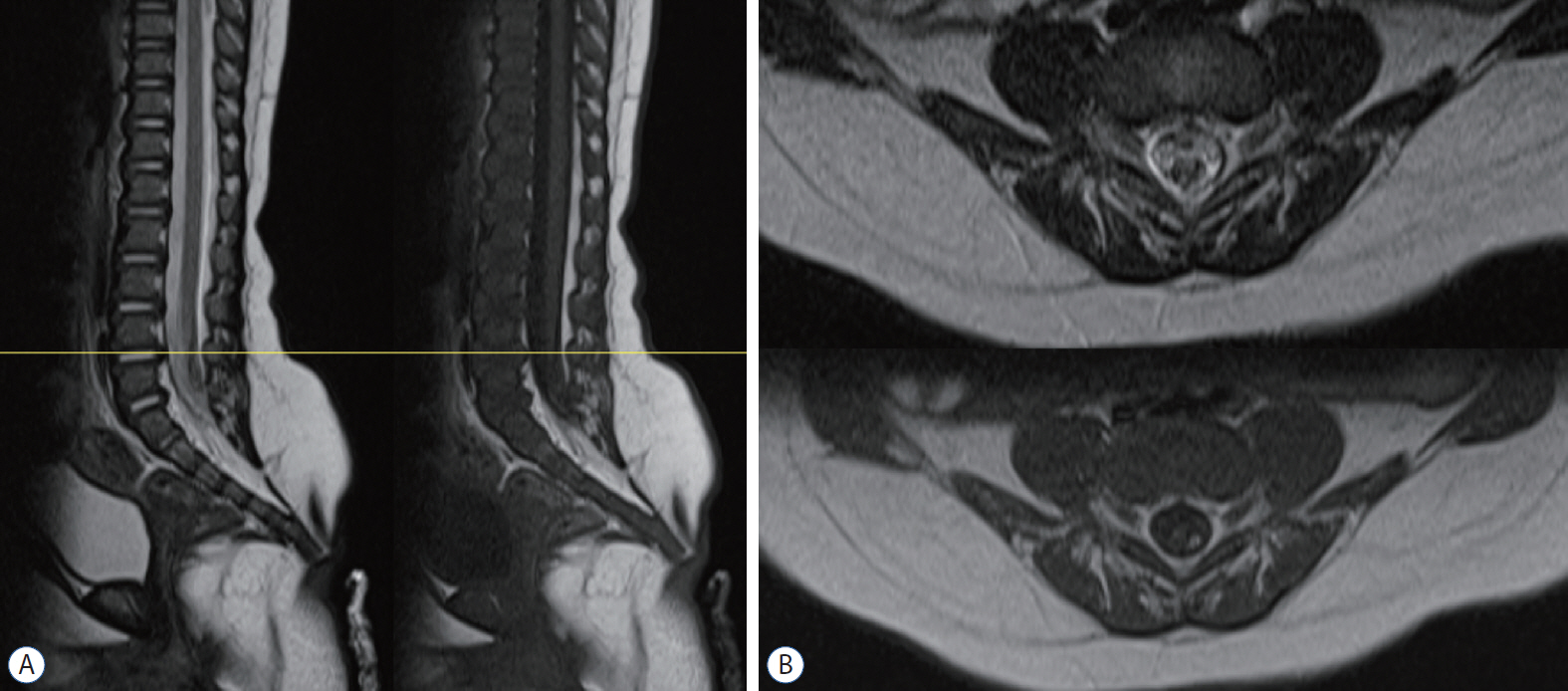
Fig. 4. MRI of an RMC patient. a : The signal intensity is indistinguishable between the spinal cord and the RMC. On operation, the non-functional part of the RMC was identified by electrophysiological monitoring and was resected. B : axial images at L4-5 (yellow line in a). MRI : magnetic resonance imaging, RMC : retained medullary cord.

Fig. 5. Magnetic resonance imaging and intraoperative photograph of a retained medullary cord patient. a : a cord-like structure extending to the sacral area. B : axial images at L5 (yellow line in a). C : The limited L5 unilateral partial hemilaminectomy shows a thick, pia-covered medullary cord passing through. D : after resection of the non-functional medullary cord. Pial reconstruction was performed at the most caudal part of the cord. Removal of the non-functional segment creates a gap and may reduce the chance of retethering compared with just cutting.
Cited by 2 articles
-
Disorders of Secondary Neurulation : Mainly Focused on Pathoembryogenesis
Jeyul Yang, Ji Yeoun Lee, Kyung Hyun Kim, Kyu-Chang Wang
J Korean Neurosurg Soc. 2021;64(3):386-405. doi: 10.3340/jkns.2021.0023.Perspectives : The Role of Clinicians in Understanding Secondary Neurulation
Kyu-Chang Wang
J Korean Neurosurg Soc. 2021;64(3):414-417. doi: 10.3340/jkns.2021.0040.
Reference
-
References
1. Borner C, Monney L, Olivier R, Rossé T, Häcki J, Conus S. Life and death in a medieval atmosphere. Cell Death Differ. 6:201–206. 1999.
Article2. Chung YN, Lee DH, Yang HJ, Kim SK, Lee YJ, Lee MS, et al. Expression of neuronal markers in the secondary neurulation of chick embryos. Childs Nerv Syst. 24:105–110. 2008.
Article3. Elmore S. Apoptosis: a review of programmed cell death. Toxicol Pathol. 35:495–516. 2007.
Article4. Griffith CM, Wiley MJ, Sanders EJ. The vertebrate tail bud: three germ layers from one tissue. Anat Embryol (Berl). 185:101–113. 1992.
Article5. Hetts SW. To die or not to die: an overview of apoptosis and its role in disease. JAMA. 279:300–307. 1998.6. Hughes AF, Freeman RB. Comparative remarks on the development of the tail cord among higher vertebrates. J Embryol Exp Morphol. 32:355–363. 1974.
Article7. Mills CL, Bellairs R. Mitosis and cell death in the tail of the chick embryo. Anat Embryol (Berl). 180:301–308. 1989.
Article8. Morioka T, Murakami N, Kanata A, Tsukamoto H, Suzuki SO. Retained medullary cord with sacral subcutaneous meningocele and congenital dermal sinus. Childs Nerv Syst. 36:423–427. 2020.
Article9. Müller F, O'Rahilly R. The development of the human brain, the closure of the caudal neuropore, and the beginning of secondary neurulation at stage 12. Anat Embryol (Berl). 176:413–430. 1987.
Article10. Müller F, O'Rahilly R. The primitive streak, the caudal eminence and related structures in staged human embryos. Cells Tissues Organs. 177:2–20. 2004.
Article11. Murakami N, Morioka T, Shimogawa T, Hashiguchi K, Mukae N, Uchihashi K, et al. Retained medullary cord extending to a sacral subcutaneous meningocele. Childs Nerv Syst. 34:527–533. 2018.
Article12. Nievelstein RA, Hartwig NG, Vermeij-Keers C, Valk J. Embryonic development of the mammalian caudal neural tube. Teratology. 48:21–31. 1993.
Article13. Nijhawan D, Honarpour N, Wang X. Apoptosis in neural development and disease. Annu Rev Neurosci. 23:73–87. 2000.
Article14. O'Rahilly R, Müller F. Neurulation in the normal human embryo. Ciba Found Symp. 181:70–82. discussion 82-89. 1994.15. Pang D, Chong S, Wang KC. Secondary Neurulation Defects-1: Thickened Filum Terminale, Retained Medullary Cord. In : Di Rocco C, Pang D, Rutka J, editors. Textbook of Pediatric Neurosurgery. Cham: Springer;2017. p. 1–18.16. Pang D, Zovickian J, Moes GS. Retained medullary cord in humans: late arrest of secondary neurulation. Neurosurgery. 68:1500–1519. discussion 1519. 2011.
Article17. Sala F, Barone G, Tramontano V, Gallo P, Ghimenton C. Retained medullary cord confirmed by intraoperative neurophysiological mapping. Childs Nerv Syst. 30:1287–1291. 2014.
Article18. Schoenwolf GC. Morphogenetic processes involved in the remodeling of the tail region of the chick embryo. Anat Embryol (Berl). 162:183–197. 1981.
Article19. Shirozu N, Morioka T, Inoha S, Imamoto N, Sasaguri T. Enlargement of sacral subcutaneous meningocele associated with retained medullary cord. Childs Nerv Syst. 34:1785–1790. 2018.
Article20. Yang HJ, Wang KC, Chi JG, Lee MS, Lee YJ, Kim SK, et al. Cytokinetics of secondary neurulation in chick embryos: Hamburger and Hamilton stages 16-45. Childs Nerv Syst. 22:567–571. 2006.
Article21. Yang HJ, Wang KC, Chi JG, Lee MS, Lee YJ, Kim SK, et al. Neural differentiation of caudal cell mass (secondary neurulation) in chick embryos: Hamburger and Hamilton stages 16-45. Brain Res Dev Brain Res. 142:31–36. 2003.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Disorders of Secondary Neurulation : Mainly Focused on Pathoembryogenesis
- Perspectives : The Role of Clinicians in Understanding Secondary Neurulation
- Overview of Secondary Neurulation
- Spinal Dysraphism in the Last Two Decades : What I Have Seen during the Era of Dynamic Advancement
- Transcriptional Signature of Valproic Acid-Induced Neural Tube Defects in Human Spinal Cord Organoids
