Duodenal Leiomyosarcoma Presenting with Gastrointestinal Bleeding and Obstruction: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea.
- 2Biomedical Research Institute, Pusan National University Hospital, Busan, Korea. doc0224@pusan.ac.kr
- 3Department of Pathology, Pusan National University School of Medicine, Busan, Korea.
- KMID: 2471148
- DOI: http://doi.org/10.4166/kjg.2020.75.2.94
Abstract
- Duodenal leiomyosarcoma is a rare condition with a poor prognosis. Early diagnosis of duodenal leiomyosarcoma is challenging because it presents with nonspecific symptoms and endoscopic biopsies usually do not enable a definitive diagnosis. Duodenal leiomyosarcomas are diagnosed on the basis of the histopathological identification of a mesenchymal lesion composed of malignant tumor cells that on immunohistochemical examination is positive for smooth muscle actin and desmin. We report the case of a 38-year-old man who presented with gastrointestinal bleeding and obstruction who was diagnosed with duodenal leiomyosarcoma after surgical resection.
MeSH Terms
Figure
-
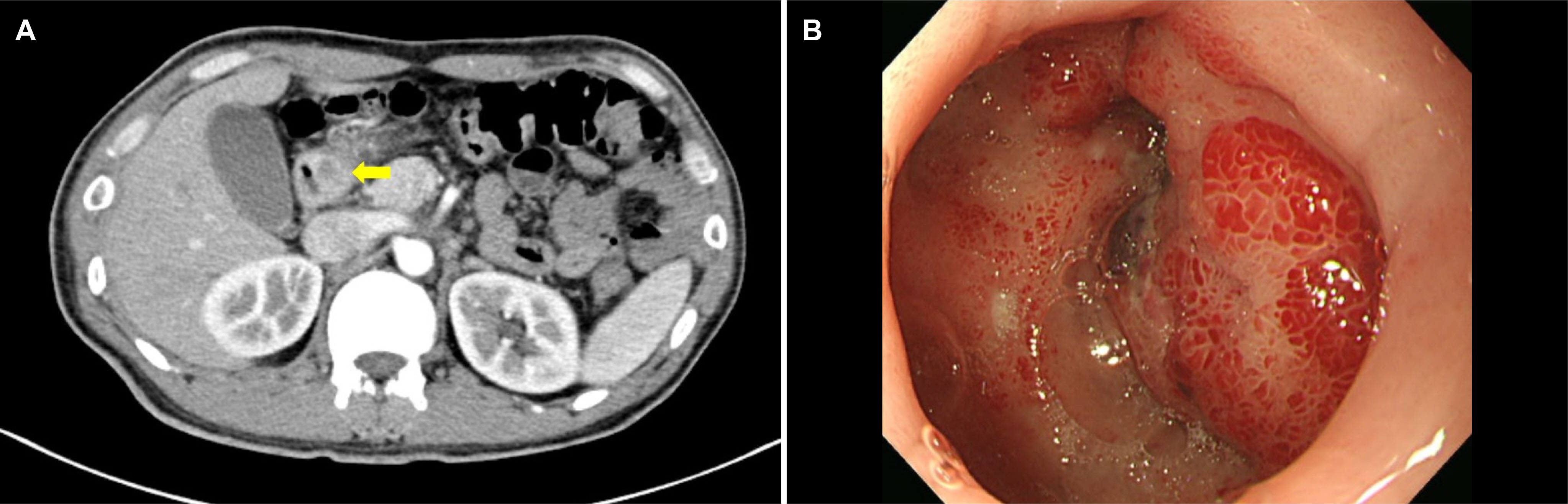
Fig. 1. (A) Contrastenhanced abdominal computed tomography image showing an ulcerative hypodense lesion at the duodenal bulb (arrow).(B) Endoscopic image showing an ulceroinfiltrative mass at the duodenal bulb nearly obstructing duodenal lumen.
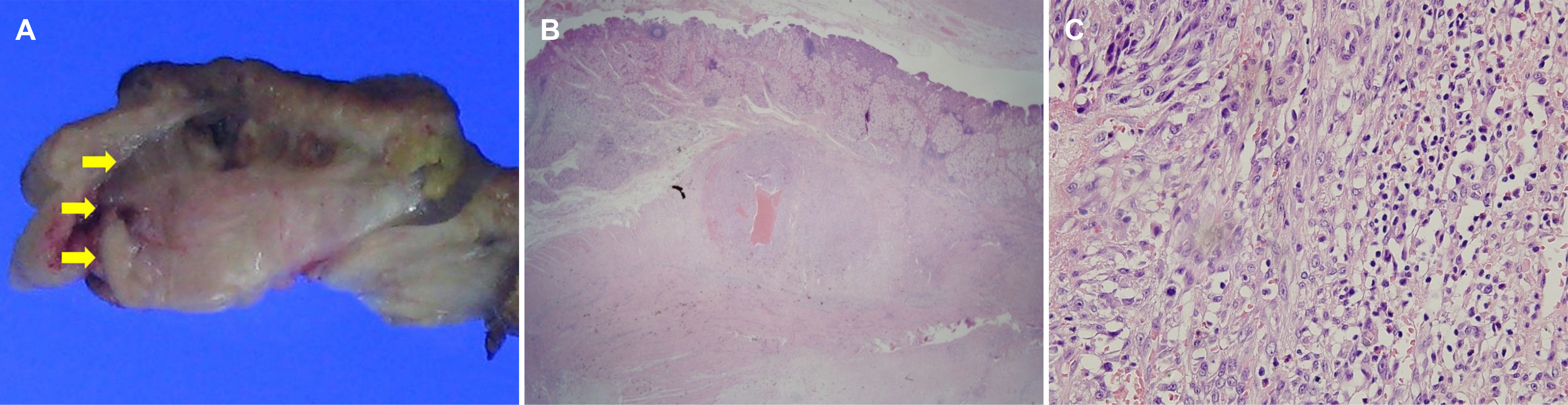
Fig. 2. (A) Macroscopic examination revealed an ill-defined, solid white mass measuring 1.6×1.0 cm in size in muscularis propria of the duodenal bulb (arrows). (B) Histopathological examination of the resected specimen showed the mass was composed of proliferating spindle cells mixed with inflammatory cells within duodenal muscularis propria (H&E, ×12.5). (C) Spindle cells showed marked pleomorphism and the mitotic count was 21/10 high-power fields (H&E, ×400).

Fig. 3. Immunohistochemical examination revealed tumor cells with immunonegative for (A) c-kit, (B) DOG-1, (C) S-100, and (D) ALK-1 and (E) immunopositive for smooth muscle actin and (F) desmin (original magnification, ×200).
Reference
-
References
1. Kang HC, Menias CO, Gaballah AH, et al. Beyond the GIST: mesenchymal tumors of the stomach. Radiographics. 2013; 33:1673–1690.
Article2. Miettinen M, Lasota J. Gastrointestinal stromal tumors–definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch. 2001; 438:1–12.3. Diamond T, Danton MH, Parks TG. Smooth muscle tumours of the alimentary tract. Ann R Coll Surg Engl. 1990; 72:316–320.4. Jerraya H, Guirat A, Frikha F, Beyrouti I. Leiomyosarcoma of the duodeno-jejunal angle: two case reports and literature review. Surg Sci. 2013; 4:313–316.
Article5. Owada Y, Haji S, Asakura R, et al. A case report of resectable leiomyosarcoma of the duodenum origin invading to the inferior vena cava. Gan To Kagaku Ryoho. 2018; 45:142–144.6. Katz SC, DeMatteo RP. Gastrointestinal stromal tumors and leiomyosarcomas. J Surg Oncol. 2008; 97:350–359.
Article7. Yeo GE, Kwon HJ, Kim JH, Chang HK, Park JG. A incidentally diagnosed duodenal subepithelial mass: gangliocytic paraganglioma treated by endoscopic mucosal resection. Korean J Helicobacter Up Gastrointest Res. 2019; 19:132–136.
Article8. Olurin EO, Solanke TF. Case of leiomyosarcoma of the duodenum and a review of the literature. Gut. 1968; 9:672–677.
Article9. Pahwa M, Girotra M, Rautela A, Goel K, Taneja S, Abraham RR. Periampullary leiomyosarcoma presenting with cutaneous metastases: a rare entity. South Med J. 2010; 103:1190–1191.
Article10. Serrano C, George S. Leiomyosarcoma. Hematol Oncol Clin North Am. 2013; 27:957–974.
Article11. Petralia GA, Hansen PD, Bowyer RC, Williamson RC. Duodenal leiomyosarcoma. Dig Surg. 1999; 16:22–25.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Duodenal Leiomyosarcoma
- A Case of Massive Upper Gastrointestinal Bleeding from a Duodenal Diverticulum
- Giant Brunner’s Gland Hamartoma of the Duodenal Bulb Presenting with Upper Gastrointestinal Bleeding and Obstruction
- A Case of Primary Leiomyosarcoma of the Liver Presenting with Acute Bleeding
- A Case of Brunner's Gland Hyperplasia of the Duodenal Second Portion with Annular Stricture Causing an Induced Obstruction
