Cone-Beam Computed Tomography-Hepatic Arteriography as a Diagnostic Tool for Small Hypervascular Hepatocellular Carcinomas: Method and Clinical Implications
- Affiliations
-
- 1Department of Radiology, Seoul National University-Seoul Metropolitan Government Boramae Medical Center, Seoul, Korea.
- 2Department of Radiology, Seoul National University Hospital, Seoul, Korea. chungjw@snu.ac.kr
- KMID: 2470754
- DOI: http://doi.org/10.3348/kjr.2019.0060
Abstract
OBJECTIVE
This study proposes a novel reference standard for hypervascular hepatocellular carcinomas (HCCs), established by cone-beam computed tomography-hepatic arteriography (CBCT-HA) and two-year imaging follow-up, and discusses its clinical implication on tumor staging and understanding the intrahepatic distant recurrence (IDR) in relation to dynamic computed tomography (CT).
MATERIALS AND METHODS
In this retrospective study, 99 patients were enrolled, who underwent CBCT-HA during initial chemoembolization for HCC suspected on CT. All patients underwent chemoembolization and regular clinical and imaging follow-up for two years. If IDR appeared on follow-up imaging, initial CBCT-HA images were reviewed to determine if a hypervascular focus pre-existed at the site of recurrence. Pre-existing hypervascular foci on CBCT-HA were regarded as HCCs in initial presentation. Initial HCCs were classified into three groups according to their mode of detection (Group I, detected on CT and CBCT-HA; Group II, additionally detected on CBCT-HA; Group III, confirmed by interval growth). We assessed the influence of CBCT-HA and two-year follow-up on initial tumor stage and calculated the proportion of IDR that pre-existed in initial CBCT-HA.
RESULTS
A total of 405 nodules were confirmed as HCCs, and 297 nodules initially pre-existed. Of the initial 297 HCCs, 149 (50.2%) lesions were in Group I, 74 (24.9%) lesions were in Group II, and the remaining 74 (24.9%) lesions were in Group III. After applying CBCT-HA findings, 11 patients upstaged in T stage, and 4 patients had a change in Milan criteria. Our reference standard for HCC indicated that 120 of 148 (81.1%) one-year IDR and 148 of 256 (57.8%) two-year IDR existed on initial CBCT-HA.
CONCLUSION
The proposed method enabled the confirmation of many sub-centimeter-sized, faintly vascularized HCC nodules that pre-existed initially but clinically manifested as IDR. Our reference standard for HCC helped in understanding the nature of IDR and the early development of HCC as well as the clinical impact of tumor staging and treatment decision.
Keyword
MeSH Terms
Figure
-
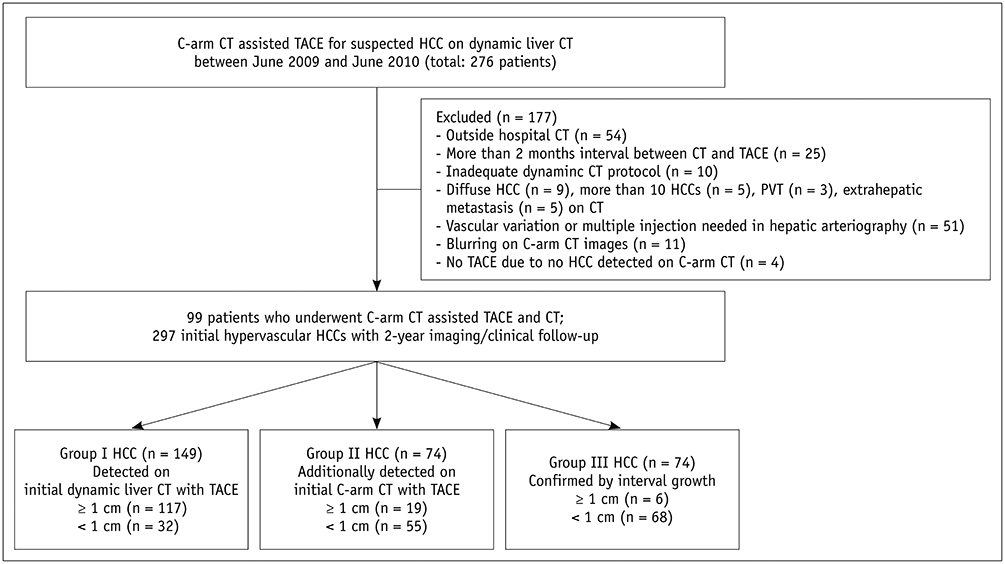
Fig. 1 Flowchart shows study group inclusion process. HCC = hepatocellular carcinoma, PVT = portal vein thrombosis, TACE = transcatheter arterial chemoembolization

Fig. 2 Number of patients with nodules in each group. n(Gr #) = number of nodules in group #
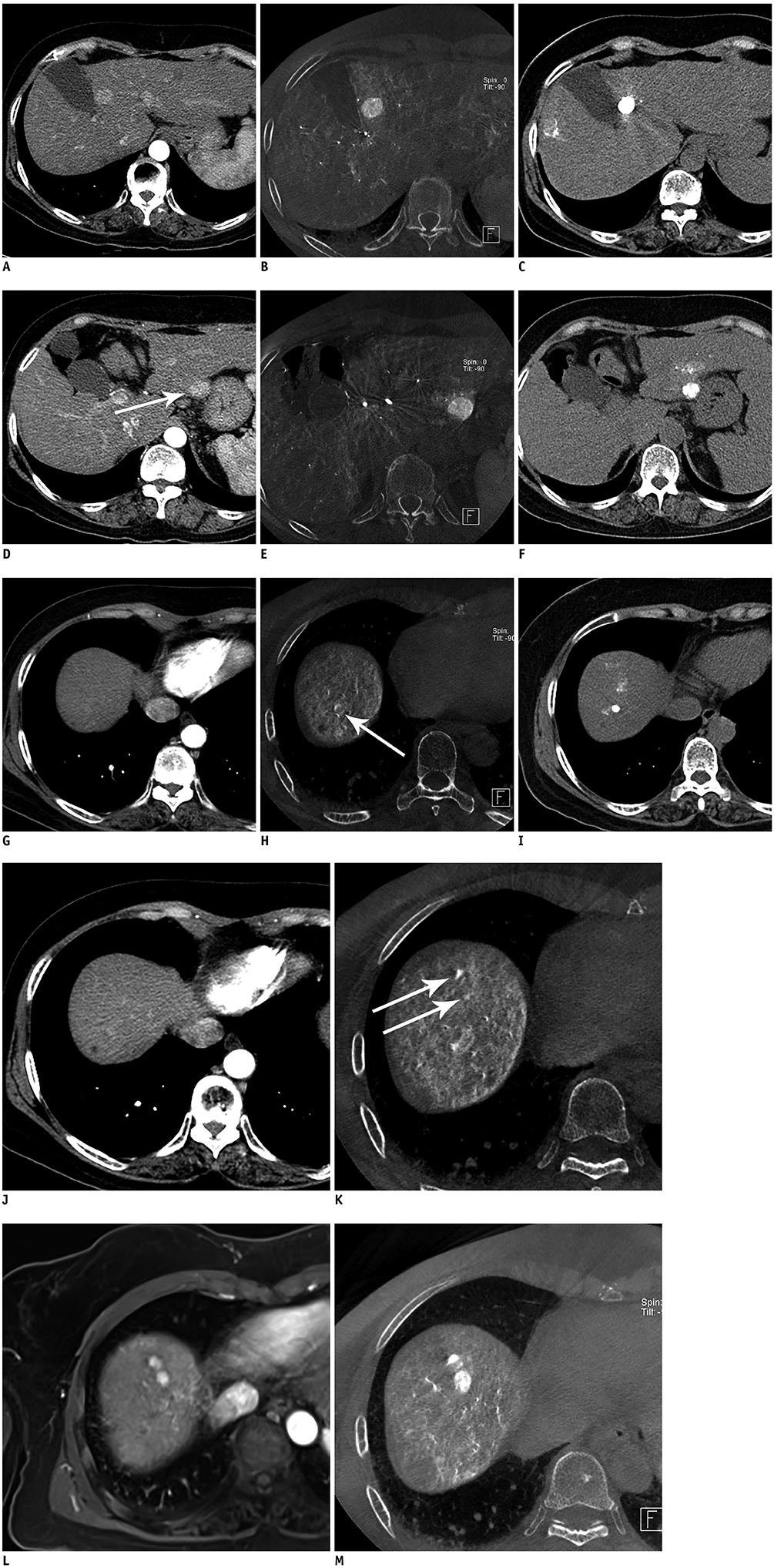
Fig. 3 62-year-old woman with overt HCCs on initial dynamic CT and multiple hidden (additional hypervascular) foci seen on CBCT-HA. (A–F; Group I) Two overt HCC lesions on initial dynamic CT (A and D [arrow] on arterial phase) revealed strongly enhancing nodules on initial CBCT-HA (B, E). They were treated with TACE and demonstrated compact Lpiodol Ultra Fluide (Laboratoire Guerbet) uptake on immediate post-TACE non-contrast CT (C, F). (G–I; Group II) Initial CBCT-HA revealed one additional enhancing nodule (arrow) (H) which was not depicted on initial dynamic CT (G). Nodule was selectively treated with TACE and demonstrated compact Lipiodol uptake on immediate post-TACE noncontrast CT. CBCT-HA = cone-beam computed tomography-hepatic arteriography (J–M; Group III) Twenty months later, two overt recurrent HCCs were found on dynamic liver MRI (L) and CBCT-HA (M). On retrospective review of initial dynamic CT (J) and CBCT-HA (K), two tiny enhancing foci (arrows) seen on initial CBCT-HA at sites match exactly with location of recurrent tumors. Follow-up CBCT-HA (M) demonstrated interval growth of those tiny enhancing foci. CBCT-HA = cone-beam computed tomography-hepatic arteriography
Reference
-
1. El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology. 2007; 132:2557–2576.
Article2. Shimizu A, Ito K, Koike S, Fujita T, Shimizu K, Matsunaga N. Cirrhosis or chronic hepatitis: evaluation of small (≤2-cm) early-enhancing hepatic lesions with serial contrast-enhanced dynamic MR imaging. Radiology. 2003; 226:550–555.
Article3. Kim JE, Kim SH, Lee SJ, Rhim H. Hypervascular hepatocellular carcinoma 1 cm or smaller in patients with chronic liver disease: characterization with gadoxetic acid-enhanced MRI that includes diffusion-weighted imaging. AJR Am J Roentgenol. 2011; 196:W758–W765.
Article4. Borzio M, Borzio F, Macchi R, Croce AM, Bruno S, Ferrari A, et al. The evaluation of fine-needle procedures for the diagnosis of focal liver lesions in cirrhosis. J Hepatol. 1994; 20:117–121.
Article5. Stigliano R, Burroughs AK. Should we biopsy each liver mass suspicious for HCC before liver transplantation?–No, please don't. J Hepatol. 2005; 43:563–568.
Article6. Tan CH, Low SCA, Thng CH. APASL and AASLD consensus guidelines on imaging diagnosis of hepatocellular carcinoma: a review. Int J Hepatol. 2011; 2011:519783.
Article7. Bhartia B, Ward J, Guthrie JA, Robinson PJ. Hepatocellular carcinoma in cirrhotic livers: double-contrast thin-section MR imaging with pathologic correlation of explanted tissue. AJR Am J Roentgenol. 2003; 180:577–584.8. Forner A, Vilana R, Ayuso C, Bianchi L, Solé M, Ayuso JR, et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology. 2008; 47:97–104.
Article9. Addley HC, Griffin N, Shaw AS, Mannelli L, Parker RA, Aitken S, et al. Accuracy of hepatocellular carcinoma detection on multidetector CT in a transplant liver population with explant liver correlation. Clin Radiol. 2011; 66:349–356.
Article10. Wald C, Russo MW, Heimbach JK, Hussain HK, Pomfret EA, Bruix J. New OPTN/UNOS policy for liver transplant allocation: standardization of liver imaging, diagnosis, classification, and reporting of hepatocellular carcinoma. Radiology. 2013; 266:376–382.
Article11. Miyayama S, Matsui O, Yamashiro M, Ryu Y, Takata H, Takeda T, et al. Detection of hepatocellular carcinoma by CT during arterial portography using a cone-beam CT technology: comparison with conventional CTAP. Abdom Imaging. 2009; 34:502–506.
Article12. Kakeda S, Korogi Y, Ohnari N, Moriya J, Oda N, Nishino K, et al. Usefulness of cone-beam volume CT with flat panel detectors in conjunction with catheter angiography for transcatheter arterial embolization. J Vasc Interv Radiol. 2007; 18:1508–1516.
Article13. Miyayama S, Yamashiro M, Okuda M, Yoshie Y, Sugimori N, Igarashi S, et al. Usefulness of cone-beam computed tomography during ultraselective transcatheter arterial chemoembolization for small hepatocellular carcinomas that cannot be demonstrated on angiography. Cardiovasc Intervent Radiol. 2009; 32:255–264.
Article14. Meyer BC, Frericks BB, Voges M, Borchert M, Martus P, Justiz J, et al. Visualization of hypervascular liver lesions during TACE: comparison of angiographic C-arm CT and MDCT. AJR Am J Roentgenol. 2008; 190:W263–W269.
Article15. Sze DY, Razavi MK, So SK, Jeffrey RB Jr. Impact of multidetector CT hepatic arteriography on the planning of chemoembolization treatment of hepatocellular carcinoma. AJR Am J Roentgenol. 2001; 177:1339–1345.
Article16. Akpek S, Brunner T, Benndorf G, Strother C. Three-dimensional imaging and cone beam volume CT in C-arm angiography with flat panel detector. Diagn Interv Radiol. 2005; 11:10–13.17. Lee IJ, Chung JW, Yin YH, Kim HC, Kim YI, Jae HJ, et al. Cone-beam CT hepatic arteriography in chemoembolization for hepatocellular carcinoma: angiographic image quality and its determining factors. J Vasc Interv Radiol. 2014; 25:1369–1379.e1.
Article18. Lee IJ, Chung JW, Yin YH, Kim HC, Kim YI, Jae HJ, et al. Cone-beam computed tomography (CBCT) hepatic arteriography in chemoembolization for hepatocellular carcinoma: performance depicting tumors and tumor feeders. Cardiovasc Intervent Radiol. 2015; 38:1218–1230.
Article19. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996; 334:693–700.
Article20. Brierley JD, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumours. 8th ed. Oxford: John Wiley & Sons, Ltd;2017.21. Higashihara H, Osuga K, Onishi H, Nakamoto A, Tsuboyama T, Maeda N, et al. Diagnostic accuracy of C-arm CT during selective transcatheter angiography for hepatocellular carcinoma: comparison with intravenous contrast-enhanced, biphasic, dynamic MDCT. Eur Radiol. 2012; 22:872–879.
Article22. Iwazawa J, Ohue S, Hashimoto N, Abe H, Hamuro M, Mitani T. Detection of hepatocellular carcinoma: comparison of angiographic C-arm CT and MDCT. AJR Am J Roentgenol. 2010; 195:882–887.
Article23. Jin YJ, Nah SY, Lee JW, Lee JI, Jeong S, Lee DH, et al. Utility of adding Primovist magnetic resonance imaging to analysis of hepatocellular carcinoma by liver dynamic computed tomography. Clin Gastroenterol Hepatol. 2013; 11:187–192.
Article24. Yoo SH, Choi JY, Jang JW, Bae SH, Yoon SK, Kim DG, et al. Gd-EOB-DTPA-enhanced MRI is better than MDCT in decision making of curative treatment for hepatocellular carcinoma. Ann Surg Oncol. 2013; 20:2893–2900.
Article25. Choi SH, Byun JH, Kwon HJ, Ha HI, Lee SJ, Kim SY, et al. The usefulness of gadoxetic acid-enhanced dynamic magnetic resonance imaging in hepatocellular carcinoma: toward improved staging. Ann Surg Oncol. 2015; 22:819–825.
Article26. El-Serag HB, Marrero JA, Rudolph L, Reddy KR. Diagnosis and treatment of hepatocellular carcinoma. Gastroenterology. 2008; 134:1752–1763.
Article27. Imamura H, Matsuyama Y, Tanaka E, Ohkubo T, Hasegawa K, Miyagawa S, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003; 38:200–207.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of C-Arm Cone-Beam CT in Chemoembolization for Hepatocellular Carcinoma
- Management of root canal perforation by using cone-beam computed tomography
- Conventional Chemoembolization for Hepatocellular Carcinoma: Role of Cone-Beam Computed Tomography Guidance
- Three-dimensional imaging modalities in endodontics
- Detection of maxillary second molar with two palatal roots using cone beam computed tomography: a case report
