Conventional Chemoembolization for Hepatocellular Carcinoma: Role of Cone-Beam Computed Tomography Guidance
- Affiliations
-
- 1Department of Radiology, National Cancer Center, Goyang, Korea.
- 2Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. chungjw@snu.ac.kr
- KMID: 2448273
- DOI: http://doi.org/10.17998/jlc.19.1.19
Abstract
- Conventional chemoembolization using Lipiodol-based regimens was introduced in the 1980s, and it is currently recommended as the primary treatment modality for patients with unresectable, intermediate, or locally advanced hepatocellular carcinoma (HCC) by the international guidelines. For better therapeutic efficacy and safety, chemoembolization should be performed as selectively as possible through tumor-feeding arteries, based on the detection of arterial supply to the HCC. With the technical advancement of flat-panel detector, cone-beam computed tomography (CBCT) is mounted on the C-arm of the angiographic machine. CBCT facilitates the detection of small occult HCCs and fine tumor-feeding arteries, recognition of extrahepatic collateral supply, navigation of a microcatheter to the target feeding arteries, prevention of non-target embolization, and intraprocedural assessment of the completeness of treatment with chemoembolization. These functions performed by CBCT ultimately improve the safety and efficacy of chemoembolization and may contribute to improving the prognosis of the patient with HCC.
Figure
-
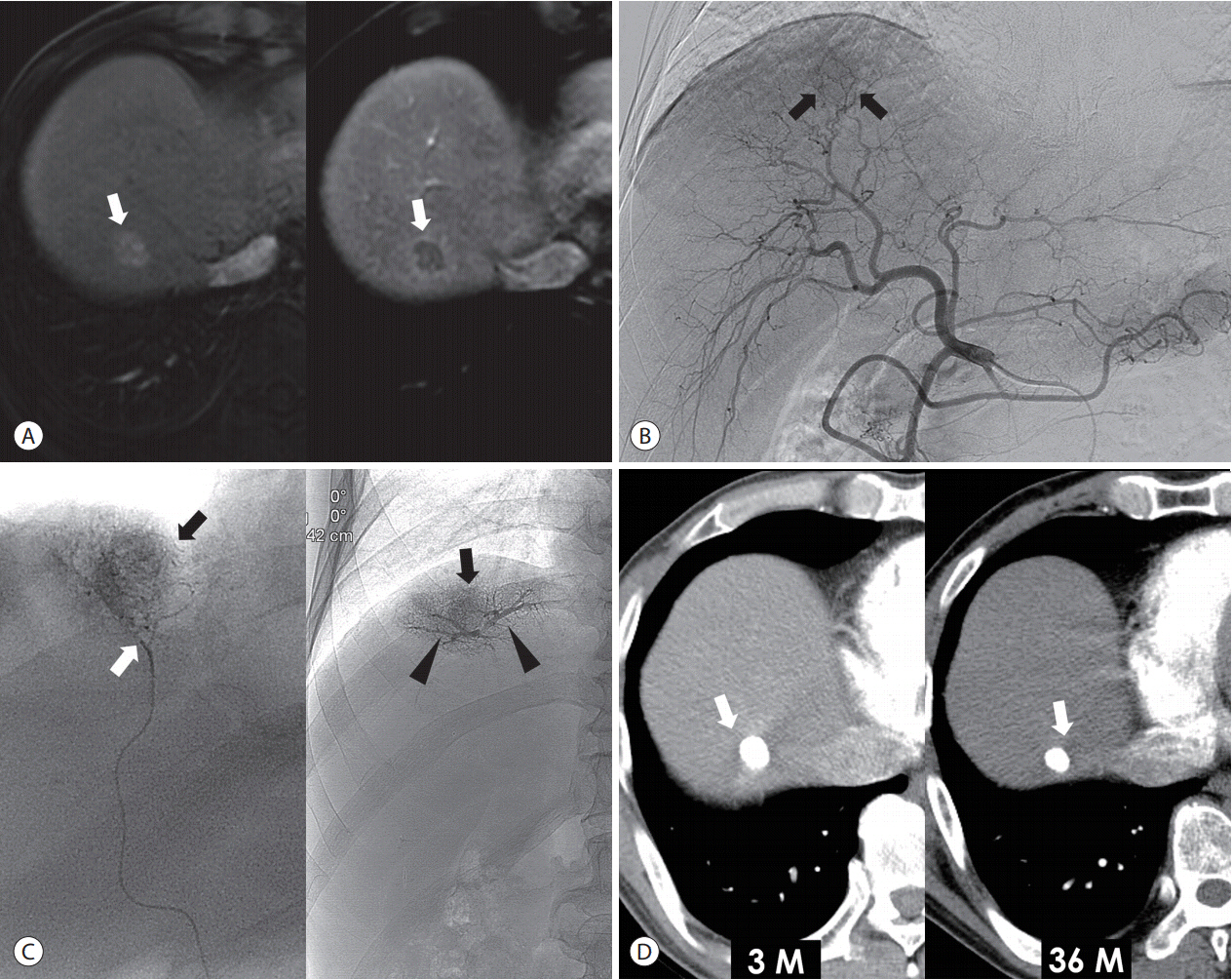
Figure 1. Superselective cTACE for a single small tumor in a 60-year-old man. (A) Liver MRI shows a 1.8 cm nodular tumor (arrows) with arterial enhancement (left side) and delayed washout (right side) in the segment 8 of the liver. (B) Common hepatic arteriography shows a faint enhancing tumor (arrows). (C) The tip (white arrow) of microcatheter is placed at the tumor-feeding artery, and the Lipiodol-based emulsion is infused. The portal veins (arrowheads) and tumor (black arrows) are visualized in the fluoroscopy image. (D) 3-month (left side) and 36-month (right side) follow-up CT shows dense Lipiodol accumulation at the tumor (arrows) without local recurrence. cTACE, conventional transarterial chemoembolization; MRI, magnetic resonance imaging; CT, computed tomography.
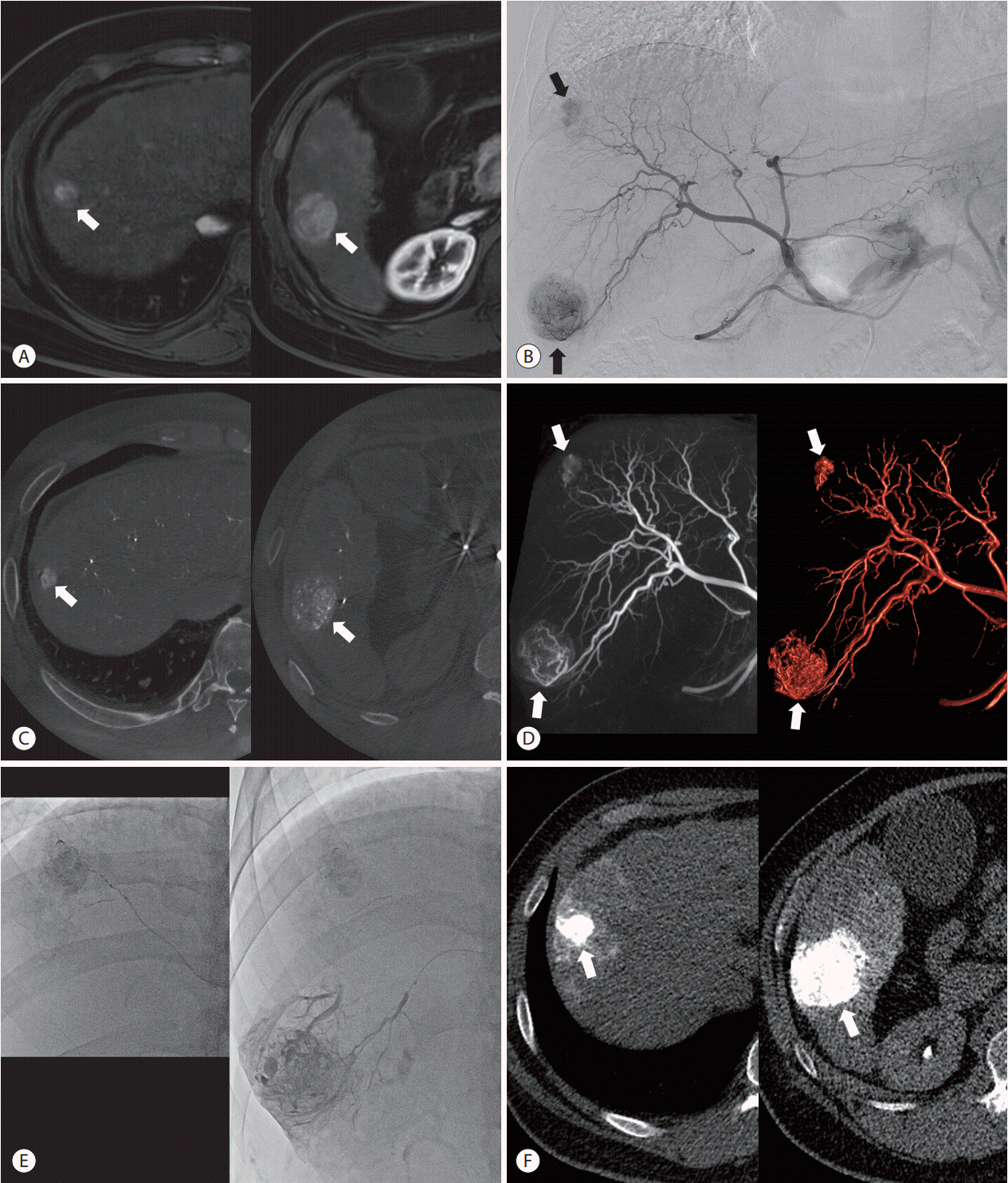
Figure 2. CBCT-guided cTACE for two nodular tumors in a 45-year-old man. (A) The arterial phase image of liver MRI shows two enhancing tumors (arrows) in segment 8 (left side) and segment 6 (right side). (B) Two enhancing tumors (arrows) are demonstrated in the common hepatic arteriography. (C) Axial image of CBCT shows two enhancing tumors (arrows) that are correlated with the preprocedural MRI. (D) The tumors (arrows) and their tumor-feeding arteries can be analyzed by using maximum intensity projection image (left side) and volume rendered image (right side). (E) Superselective chemoembolization is performed through each tumor-feeding artery. (F) Immediate, unenhanced CT shows dense Lipiodol accumulation in the tumors (arrows). CBCT, conebeam computed tomography; cTACE, conventional transarterial chemoembolization; MRI, magnetic resonance imaging; CT, computed tomography.
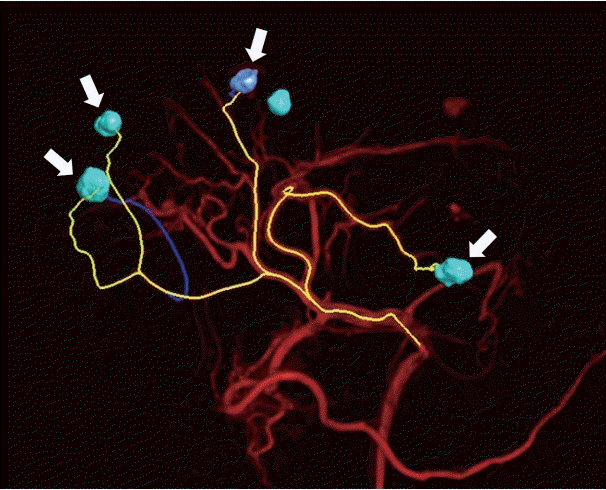
Figure 3. Depiction of the tumor-feeding arteries of four nodular tumors (arrows) using automated vessel tracking system (Emboguide; Phillips Medical Systems, Eindhoven, the Netherlands) in a 61-year-old woman.
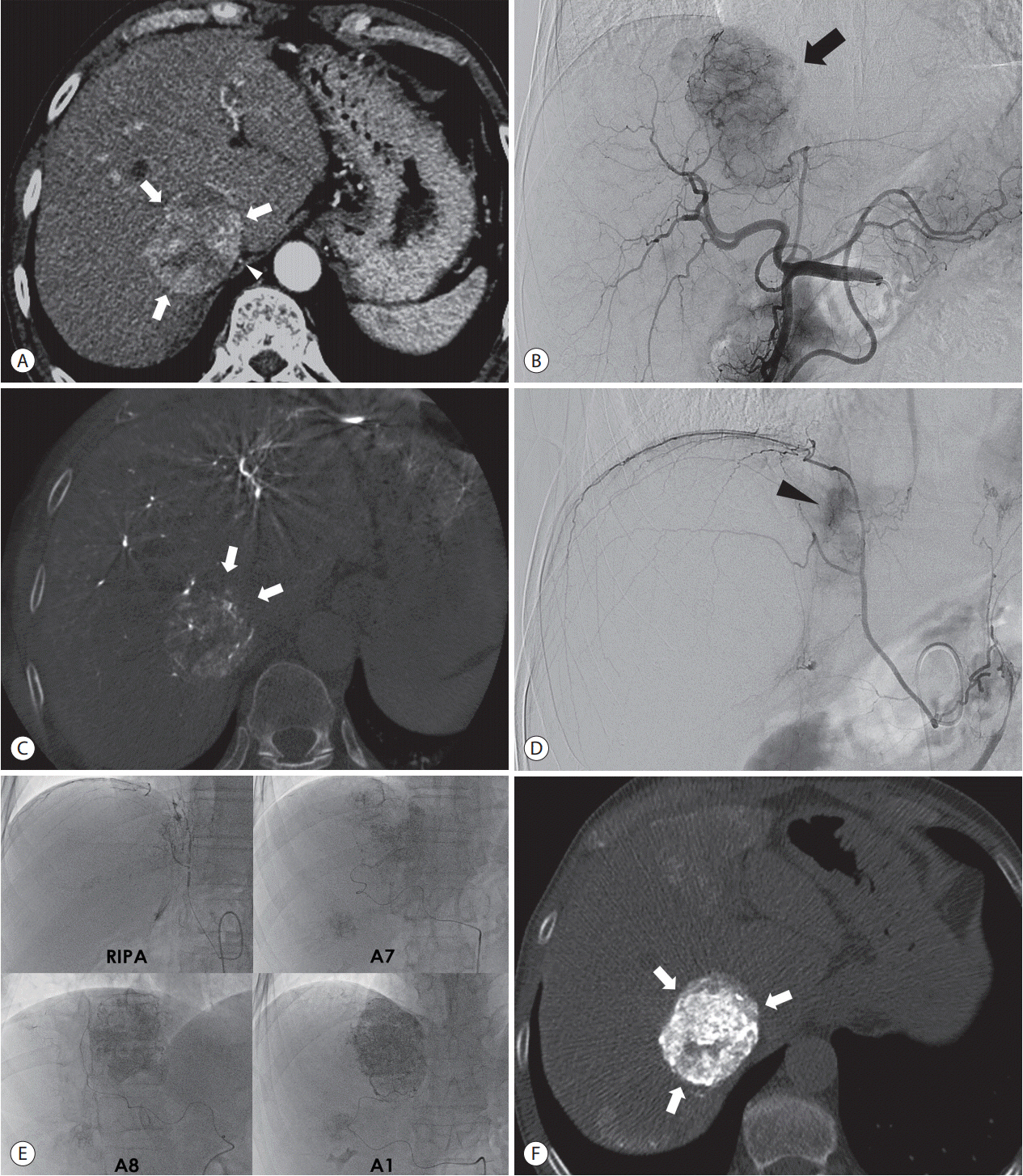
Figure 4. Recognition of extrahepatic collateral arterial supply to the tumor using CBCT images in a 62-year-old man. (A) Arterial phase image of CT shows large hypervascular tumor (arrows) in the paracaval portion of the liver. The RIPA is also demonstrated around the tumor (arrowhead). (B) Common hepatic angiography shows the hypervascular tumor (arrow). (C) Non-enhancing part (arrows) of the tumor is demonstrated in the axial image of CBCT but not in the preprocedural CT image (Fig. 4A), which suggests the presence of extrahepatic collateral artery supplying the tumor. (D) Angiography of the RIPA shows tumor staining. Angiography of the RIPA shows tumor staining (arrowhead). (E) Supserselective cTACE is performed through the RIPA, segment 7 hepatic artery, segment 8 hepatic artery, and caudate artery. (F) Immediate, unenhanced CT shows dense Lipiodol accumulation at the tumor (arrows). CBCT, cone-beam computed tomography; CT, computed tomography; RIPA, right inferior phrenic artery; cTACE, conventional transarterial chemoembolization.

Figure 5. Recognition of extrahepatic collateral arterial supply to the small tumor using CBCT images in a 55-year-old man. (A) Arterial phase image of MRI shows a small-rim enhancing tumor (arrow) at the paracaval portion of the liver. (B) On distal subtraction angiography of the common hepatic arteriography (left side), it is difficult to know whether or not there is tumor staining. However, the axial image of CBCT (right side) shows no tumor staining and the parenchymal perfusion defect at the paracaval portion (circle), which suggests the presence of an extrahepatic collateral arterial supply. This is the typical location that is supplied by the right inferior phrencic artery. (C) Tumor staining (arrow on left side) is suspected on distal subtraction angiography of the right inferior phrenic arteriography, but it is difficult to be sure. However, the axial image of CBCT clearly shows the small tumor (arrow on right), which is detected with preprocedural MRI. CBCT, cone-beam computed tomography; MRI, magnetic resonance imaging.
Reference
-
1. Llovet JM, Real MI, Montaña X, Planas R, Coll S, Aponte J, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002; 359:1734–1739.2. Lo CM, Ngan H, Tso WK, Liu CL, Lam CM, Poon RT, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002; 35:1164–1171.3. Korean Liver Cancer Study Group (KLCSG); National Cancer Center, Korea (NCC). 2014 Korean Liver Cancer Study Group-National Cancer Center Korea practice guideline for the management of hepatocellular carcinoma. Korean J Radiol. 2015; 16:465–522.4. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018; 69:182–236.5. Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018; 67:358–380.6. Yau T, Tang VY, Yao TJ, Fan ST, Lo CM, Poon RT. Development of Hong Kong Liver Cancer staging system with treatment stratification for patients with hepatocellular carcinoma. Gastroenterology. 2014; 146:1691–1700. e3.7. Park JW, Chen M, Colombo M, Roberts LR, Schwartz M, Chen PJ, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015; 35:2155–2166.8. Golfieri R, Cappelli A, Cucchetti A, Piscaglia F, Carpenzano M, Peri E, et al. Efficacy of selective transarterial chemoembolization in inducing tumor necrosis in small (<5 cm) hepatocellular carcinomas. Hepatology. 2011; 53:1580–1589.9. Golfieri R, Renzulli M, Mosconi C, Forlani L, Giampalma E, Piscaglia F, et al. Hepatocellular carcinoma responding to superselective transarterial chemoembolization: an issue of nodule dimension? J Vasc Interv Radiol. 2013; 24:509–517.10. Takaki S, Sakaguchi H, Anai H, Tanaka T, Yamamoto K, Morimoto K, et al. Long-term outcome of transcatheter subsegmental and segmental arterial chemoemobolization using lipiodol for hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2012; 35:544–554.11. Gupta R, Grasruck M, Suess C, Bartling SH, Schmidt B, Stierstorfer K, et al. Ultra-high resolution flat-panel volume CT: fundamental principles, design architecture, and system characterization. Eur Radiol. 2006; 16:1191–1205.12. Orth RC, Wallace MJ, Kuo MD; Technology Assessment Committee of the Society of Interventional R. C-arm cone-beam CT: general principles and technical considerations for use in interventional radiology. J Vasc Interv Radiol. 2008; 19:814–820.13. Kim HC. Role of C-arm cone-beam CT in chemoembolization for hepatocellular carcinoma. Korean J Radiol. 2015; 16:114–124.14. Matsui O, Kobayashi S, Sanada J, Kouda W, Ryu Y, Kozaka K, et al. Hepatocelluar nodules in liver cirrhosis: hemodynamic evaluation (angiography-assisted CT) with special reference to multi-step hepatocarcinogenesis. Abdom Imaging. 2011; 36:264–272.15. Sasaki A, Kai S, Iwashita Y, Hirano S, Ohta M, Kitano S. Microsatellite distribution and indication for locoregional therapy in small hepatocellular carcinoma. Cancer. 2005; 103:299–306.16. Kan Z, Ivancev K, Hägerstrand I, Chuang VP, Lunderquist A. In vivo microscopy of the liver after injection of Lipiodol into the hepatic artery and portal vein in the rat. Acta Radiol. 1989; 30:419–425.17. Kan Z, Sato M, Ivancev K, Uchida B, Hedgpeth P, Lunderquist A, et al. Distribution and effect of iodized poppyseed oil in the liver after hepatic artery embolization: experimental study in several animal species. Radiology. 1993; 186:861–866.18. Kitao A, Zen Y, Matsui O, Gabata T, Nakanuma Y. Hepatocarcinogenesis: multistep changes of drainage vessels at CT during arterial portography and hepatic arteriography--radiologic-pathologic correlation. Radiology. 2009; 252:605–614.19. Miyayama S, Matsui O, Yamashiro M, Ryu Y, Kaito K, Ozaki K, et al. Ultraselective transcatheter arterial chemoembolization with a 2-f tip microcatheter for small hepatocellular carcinomas: relationship between local tumor recurrence and visualization of the portal vein with iodized oil. J Vasc Interv Radiol. 2007; 18:365–376.20. Iwamoto S, Yamaguchi T, Hongo O, Iwamoto H, Sanefuji H. Excellent outcomes with angiographic subsegmentectomy in the treatment of typical hepatocellular carcinoma: a retrospective study of local recurrence and long-term survival rates in 120 patients with hepatocellular carcinoma. Cancer. 2010; 116:393–399.21. Kalender WA, Kyriakou Y. Flat-detector computed tomography (FD-CT). Eur Radiol. 2007; 17:2767–2779.22. Virmani S, Ryu RK, Sato KT, Lewandowski RJ, Kulik L, Mulcahy MF, et al. Effect of C-arm angiographic CT on transcatheter arterial chemoembolization of liver tumors. J Vasc Interv Radiol. 2007; 18:1305–1309.23. Iwazawa J, Ohue S, Mitani T, Abe H, Hashimoto N, Hamuro M, et al. Identifying feeding arteries during TACE of hepatic tumors: comparison of C-arm CT and digital subtraction angiography. AJR Am J Roentgenol. 2009; 192:1057–1063.24. Meyer BC, Witschel M, Frericks BB, Voges M, Hopfenmüller W, Wolf KJ, et al. The value of combined soft-tissue and vessel visualisation before transarterial chemoembolisation of the liver using Carm computed tomography. Eur Radiol. 2009; 19:2302–2309.25. Lee IJ, Chung JW, Yin YH, Kim HC, Kim YI, Jae HJ, et al. Conebeam CT hepatic arteriography in chemoembolization for hepatocellular carcinoma: angiographic image quality and its determining factors. J Vasc Interv Radiol. 2014; 25:1369–1379. ; quiz 1379-.e1.26. Tognolini A, Louie J, Hwang G, Hofmann L, Sze D, Kothary N. Carm computed tomography for hepatic interventions: a practical guide. J Vasc Interv Radiol. 2010; 21:1817–1823.27. Meyer BC, Frericks BB, Voges M, Borchert M, Martus P, Justiz J, et al. Visualization of hypervascular liver lesions during TACE: comparison of angiographic C-arm CT and MDCT. AJR Am J Roentgenol. 2008; 190:W263–W269.28. Iwazawa J, Ohue S, Hashimoto N, Abe H, Hamuro M, Mitani T. Detection of hepatocellular carcinoma: comparison of angiographic C-arm CT and MDCT. AJR Am J Roentgenol. 2010; 195:882–887.29. Yu MH, Kim JH, Yoon JH, Kim HC, Chung JW, Han JK, et al. Role of C-arm CT for transcatheter arterial chemoembolization of hepatocellular carcinoma: diagnostic performance and predictive value for therapeutic response compared with gadoxetic acid-enhanced MRI. AJR Am J Roentgenol. 2013; 201:675–683.30. Bruix J, Castells A, Bosch J, Feu F, Fuster J, Garcia-Pagan JC, et al. Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology. 1996; 111:1018–1022.31. Chen RX, Gan YH, Ge NL, Chen Y, Ma H, Wang Y, et al. Comparison of transarterial chemoembolization with radiofrequency ablation for unresectable Barcelona Clinic Liver Cancer stage 0/A hepatocellular carcinoma: a propensity score matching. J Gastroenterol Hepatol. 2016; 31:442–449.32. Yang HJ, Lee JH, Lee DH, Yu SJ, Kim YJ, Yoon JH, et al. Small single-nodule hepatocellular carcinoma: comparison of transarterial chemoembolization, radiofrequency ablation, and hepatic resection by using inverse probability weighting. Radiology. 2014; 271:909–918.33. Miyayama S, Yamashiro M, Okuda M, Yoshie Y, Sugimori N, Igarashi S, et al. Usefulness of cone-beam computed tomography during ultraselective transcatheter arterial chemoembolization for small hepatocellular carcinomas that cannot be demonstrated on angiography. Cardiovasc Intervent Radiol. 2009; 32:255–264.34. Choi JW, Kim HC, Lee JH, Yu SJ, Cho EJ, Kim MU, et al. Cone beam CT-guided chemoembolization of probable hepatocellular carcinomas smaller than 1 cm in patients at high risk of hepatocellular carcinoma. J Vasc Interv Radiol. 2017; 28:795–803. e1.35. Lee IJ, Chung JW, Yin YH, Kim HC, Kim YI, Jae HJ, et al. Conebeam computed tomography (CBCT) hepatic arteriography in chemoembolization for hepatocellular carcinoma: performance depicting tumors and tumor feeders. Cardiovasc Intervent Radiol. 2015; 38:1218–1230.36. Pung L, Ahmad M, Mueller K, Rosenberg J, Stave C, Hwang GL, et al. The role of cone-beam CT in transcatheter arterial chemoembolization for hepatocellular carcinoma: a systematic review and meta-analysis. J Vasc Interv Radiol. 2017; 28:334–341.37. Deschamps F, Solomon SB, Thornton RH, Rao P, Hakime A, Kuoch V, et al. Computed analysis of three-dimensional cone-beam computed tomography angiography for determination of tumorfeeding vessels during chemoembolization of liver tumor: a pilot study. Cardiovasc Intervent Radiol. 2010; 33:1235–1242.38. Iwazawa J, Ohue S, Hashimoto N, Muramoto O, Mitani T. Clinical utility and limitations of tumor-feeder detection software for liver cancer embolization. Eur J Radiol. 2013; 82:1665–1671.39. Miyayama S, Yamashiro M, Hashimoto M, Hashimoto N, Ikuno M, Okumura K, et al. Identification of small hepatocellular carcinoma and tumor-feeding branches with cone-beam CT guidance technology during transcatheter arterial chemoembolization. J Vasc Interv Radiol. 2013; 24:501–508.40. Chung JW, Kim HC, Yoon JH, Lee HS, Jae HJ, Lee W, et al. Transcatheter arterial chemoembolization of hepatocellular carcinoma: prevalence and causative factors of extrahepatic collateral arteries in 479 patients. Korean J Radiol. 2006; 7:257–266.41. Kim HC, Chung JW, Lee W, Jae HJ, Park JH. Recognizing extrahepatic collateral vessels that supply hepatocellular carcinoma to avoid complications of transcatheter arterial chemoembolization. Radiographics. 2005; 25 Suppl 1:S25–S39.42. Moustafa AS, Abdel Aal AK, Ertel N, Saad N, DuBay D, Saddekni S. Chemoembolization of hepatocellular carcinoma with extrahepatic collateral blood supply: anatomic and technical considerations. Radiographics. 2017; 37:963–977.43. Song SY, Chung JW, Lim HG, Park JH. Nonhepatic arteries originating from the hepatic arteries: angiographic analysis in 250 patients. J Vasc Interv Radiol. 2006; 17:461–469.44. Miyayama S, Yamashiro M, Hashimoto M, Hashimoto N, Ikuno M, Okumura K, et al. Comparison of local control in transcatheter arterial chemoembolization of hepatocellular carcinoma ≤6 cm with or without intraprocedural monitoring of the embolized area using cone-beam computed tomography. Cardiovasc Intervent Radiol. 2014; 37:388–395.45. Iwazawa J, Ohue S, Hashimoto N, Muramoto O, Mitani T. Survival after C-arm CT-assisted chemoembolization of unresectable hepatocellular carcinoma. Eur J Radiol. 2012; 81:3985–3992.46. Kothary N, Abdelmaksoud MH, Tognolini A, Fahrig R, Rosenberg J, Hovsepian DM, et al. Imaging guidance with C-arm CT: prospective evaluation of its impact on patient radiation exposure during transhepatic arterial chemoembolization. J Vasc Interv Radiol. 2011; 22:1535–1543.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of C-Arm Cone-Beam CT in Chemoembolization for Hepatocellular Carcinoma
- Detection of Recurrent/Residual Hepatocellular Carcinoma: Single-Center Retrospective Comparative Study Between Parenchymal Blood Volume Mapping Using Cone Beam CT and Multiphase Dynamic CT
- Three-dimensional imaging modalities in endodontics
- Rapid Intra-Hepatic Dissemination of Hepatocellular Carcinoma with Pulmonary Metastases Following Combined Loco-Regional Therapy
- Management of root canal perforation by using cone-beam computed tomography
