Serial Magnetic Resonance Imaging Findings in Hyperglycemia-Related Osmotic Demyelination Syndrome: A Case Report
- Affiliations
-
- 1Department of Radiology, Myongji Hospital, Hanyang University College of Medicine, Goyang, Korea. nhpark@mjh.or.kr
- KMID: 2469201
- DOI: http://doi.org/10.3348/jksr.2020.81.1.243
Abstract
- We report a rare case of hyperglycemia-related osmotic demyelination syndrome (ODS) with focus on the imaging findings. A 61-year-old man with diabetes was admitted for general weakness and severe thirst. A few days later, he complained of dysarthria, dysphasia, and dysmetria. Laboratory examinations showed significant hyperglycemia, but normal electrolyte levels. Brain MRI revealed T2-signal abnormalities that were symmetrical, non-space occupying, and located in the central pons with a peripheral sparing pattern, which were suggestive of ODS. In addition, subsequent MRI revealed progression of signal hyperintensity; however, the patient's symptoms improved.
MeSH Terms
Figure
-
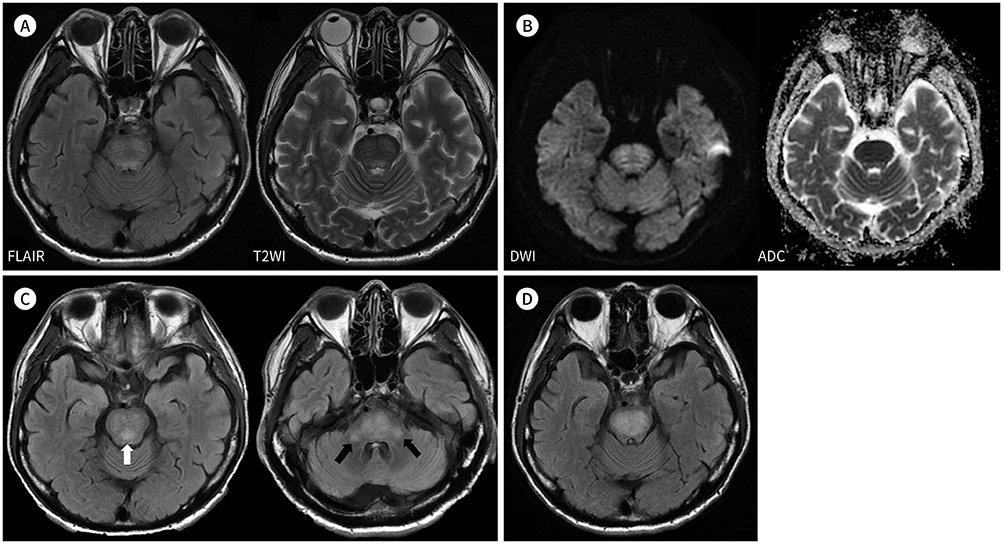
Fig. 1 Serial MR findings of hyperglycemia-related osmotic demyelination syndrome in a 61-year-old man. A. Axial FLAIR and T2WI at the level of the pons reveal bilaterally symmetric high signal intensity in the central pons with sparing of the outer rim. B. DWI and ADC map at the level of the pons reveal signal abnormalities in the affected region. On the ADC map, there is no signal dropout in the region of hyperintensity, which is consistent with T2 shine-through. C. Follow-up MRI 10 days later. Axial FLAIR MRI at the level of the upper (left) and lower pons (right) reveal newly developed high signal intensity in the posterior tegmentum area (white arrow) and bilateral brachium pontis (black arrows). D. Follow-up MRI 1 month later. Axial FLAIR MRI at the level of the upper pons demonstrates no newly developed lesions; however, the previously detected signal abnormalities have become more conspicuous and confluent. ADC = apparent diffusion coefficient, DWI = diffusion-weighted imaging, FLAIR = fluid-attenuated inversion recovery, T2WI = T2-weighted image
Reference
-
1. O'Malley G, Moran C, Draman MS, King T, Smith D, Thompson CJ, et al. Central pontine myelinolysis complicating treatment of the hyperglycaemic hyperosmolar state. Ann Clin Biochem. 2008; 45:440–443.2. Burns JD, Kosa SC, Wijdicks EF. Central pontine myelinolysis in a patient with hyperosmolar hyperglycemia and consistently normal serum sodium. Neurocrit Care. 2009; 11:251–254.
Article3. Adams RD, Victor M, Mancall EL. Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholic and malnourished patients. AMA Arch Neurol Psychiatry. 1959; 81:154–172.4. Martin RJ. Central pontine and extrapontine myelinolysis: the osmotic demyelination syndromes. J Neurol Neurosurg Psychiatry. 2004; 75 Suppl 3:iii22–iii28.
Article5. Hirosawa T, Shimizu T. Osmotic demyelination syndrome due to hyperosmolar hyperglycemia. Cleve Clin J Med. 2018; 85:511–513.
Article6. Saini M, Mamauag MJ, Singh R. Central pontine myelinolysis: a rare presentation secondary to hyperglycaemia. Singapore Med J. 2015; 56:e71–e73.
Article7. Chang YM. Central pontine myelinolysis associated with diabetic hyperglycemia. JSM Clin Case Rep. 2014; 2:1059.8. Rodríguez-Velver KV, Soto-Garcia AJ, Zapata-Rivera MA, Montes-Villarreal J, Villarreal-Pérez JZ, Rodríguez-Gutiérrez R. Osmotic demyelination syndrome as the initial manifestation of a hyperosmolar hyperglycemic state. Case Rep Neurol Med. 2014; 2014:652523.
Article9. Linyu N, Das BR, Mossang K, Singh SR, Prasad L, Naorem S. Osmotic demyelination syndrome occurs early in the course of hyperosmolar Hyperglycemic state. IOSR-JDMS. 2017; 16:25–22.10. Osborn AG, Salzman KL, Jhaveri MD, Barkovich AJ. Diagnostic imaging: brain. 3rd ed. Philadelphia: Elsevier;2015.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cortical Laminar Necrosis associated with Osmotic Demyelination Syndrome
- Osmotic Demyelination Syndrome with Recent Chemotherapy in Normonatremic Patient: A Case Report
- Characteristic Magnetic Resonance Imaging Findings of Osmotic Demyelination Syndrome in a Patient with Minimal Hyponatremia
- A Case of Osmotic Demyelination Presenting with Severe Hypernatremia
- Dynamic Contrast-Enhanced MR Imaging of Tietze’s Syndrome: a Case Report
