Pierre Robin sequence with severe scoliosis in an adult: A case report of clinical and radiological features
- Affiliations
-
- 1Department of Orthodontics, College of Dentistry, Gangneung-Wonju National University, Gangneung, Korea. korth@gwnu.ac.kr
- 2Department of Oral and Maxillofacial Radiology, College of Dentistry, Gangneung-Wonju National University, Gangneung, Korea. xraypark@gwnu.ac.kr
- KMID: 2466556
- DOI: http://doi.org/10.5624/isd.2019.49.4.323
Abstract
- Pierre Robin sequence (PRS) is characterized by the triad of micrognathia, glossoptosis, and airway obstruction. PRS does not have a single pathogenesis, but rather is associated with multiple syndromes. This report presents the case of a 35-year-old woman with PRS and scoliosis. Among the syndromes related to PRS, cerebro-costo-mandibular syndrome (CCMS), which is characterized by posterior rib gap defects and vertebral anomalies, was suspected in this patient. However, no posterior rib gap defect was detected on radiological examinations. Although over 80 cases of CCMS have been reported to date, few cases of PRS with scoliosis alone have been reported. Therefore, this report demonstrated the clinical, radiological, and cephalometric characteristics of an adult patient with PRS and scoliosis, but without rib anomalies.
Keyword
MeSH Terms
Figure
-

Fig. 1 Intraoral photos of the patient show an anterior open bite and a Class II canine relationship.

Fig. 2 A. Tongue-tie restraining the forward and upward movement of the tongue. B. Soft palate scar caused by palate surgery.
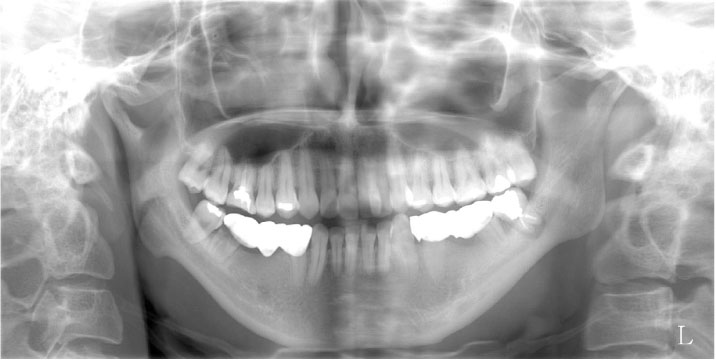
Fig. 3 A panoramic radiograph reveals deep antegonial notches, posterior bowing, and a small anteroposterior width of the bilateral condyles.

Fig. 4 A lateral cephalogram shows a small and retruded mandible, a large inclination of the mandibular plane, and a narrow airway.

Fig. 5 Superimposition of the profilograms of the patient (dotted) and normal control (solid) shows severe micrognathia and a large mandibular plane angle.

Fig. 6 Cone-beam computed tomography (CBCT) images. A-D. Three-dimensional reconstructed CBCT images demonstrate mandibular retrusion, asymmetry, and low-set ears. E and F. Coronal and axial CBCT images of the posterior soft palate area show discontinuity of the nasal septum. Note the lack of soft tissue in the posterior nasal spine area.

Fig. 7 A posteroanterior chest radiograph shows severe scoliosis and the presence of titanium rods without any signs of posterior rib gap defects.
Reference
-
1. Robin P. La chute de la base de la langue considérée comme une nouvelle cause de gêne dans la respiration nasopharyngienne. Bull Acad Med (Paris). 1923; 89:37–40.2. Tan TY, Kilpatrick N, Farlie PG. Developmental and genetic perspectives on Pierre Robin sequence. Am J Med Genet C Semin Med Genet. 2013; 163C:295–305.
Article3. Izumi K, Konczal LL, Mitchell AL, Jones MC. Underlying genetic diagnosis of Pierre Robin sequence: retrospective chart review at two children’s hospitals and a systematic literature review. J Pediatr. 2012; 160:645–650.e2.
Article4. Smith DW, Theiler K, Schachenmann G. Rib-gap defect with micrognathia, malformed tracheal cartilages, and redundant skin: a new pattern of defective development. J Pediatr. 1966; 69:799–803.
Article5. Tooley M, Lynch D, Bernier F, Parboosingh J, Bhoj E, Zackai E, et al. Cerebro-costo-mandibular syndrome: clinical, radiological, and genetic findings. Am J Med Genet A. 2016; 170A:1115–1126.
Article6. Miller KE, Allen RP, Davis WS. Rib gap defects with micrognathia. The cerebro-costo-mandibular syndrome - a Pierre Robin-like syndrome with rib dysplasia. Am J Roentgenol Radium Ther Nucl Med. 1972; 114:253–256.7. Smith KG, Sekar KC. Cerebrocostomandibular syndrome. Case report and literature review. Clin Pediatr (Phila). 1985; 24:223–225.8. Rymer AN, Porteous GH, Neal JM. Anesthetic challenges in an adult with Pierre Robin sequence, severe juvenile scoliosis, and respiratory failure. A A Case Rep. 2015; 5:95–98.
Article9. Kim JH, Gansukh O, Amarsaikhan B, Lee SJ, Kim TW. Comparison of cephalometric norms between Mongolian and Korean adults with normal occlusions and well-balanced profiles. Korean J Orthod. 2011; 41:42–50.
Article10. Kim MS, Lee EJ, Song IJ, Lee JS, Kang BC, Yoon SJ. The location of midfacial landmarks according to the method of establishing the midsagittal reference plane in three-dimensional computed tomography analysis of facial asymmetry. Imaging Sci Dent. 2015; 45:227–232.
Article11. Nah KS. Condylar bony changes in patients with temporomandibular disorders: a CBCT study. Imaging Sci Dent. 2012; 42:249–253.
Article12. Ogasawara K, Honda Y, Hosoya M. Ex utero intrapartum treatment for an infant with cerebro-costo-mandibular syndrome. Pediatr Int. 2014; 56:613–615.13. Matić A, Velisavljev-Filipović G, Lovrenski J, Gajdobranski D. A case of severe type of cerebro-costo-mandibular syndrome. Srp Arh Celok Lek. 2016; 144:431–435.
Article14. Leroy JG, Devos EA, Vanden Bulcke LJ, Robbe NS. Cerebro-costo-mandibular syndrome with autosomal dominant inheritance. J Pediatr. 1981; 99:441–443.
Article15. Merlob P, Schonfeld A, Grunebaum M, Mor N, Reisner SH. Autosomal dominant cerebro-costo-mandibular syndrome: ultrasonographic and clinical findings. Am J Med Genet. 1987; 26:195–202.
Article16. Silverman FN, Strefling AM, Stevenson DK, Lazarus J. Cerebro-costo-mandibular syndrome. J Pediatr. 1980; 97:406–416.
Article17. Lee SS, You DS. Radiographic study on maxillary sinus development and nasal septum deviation in cleft palate patient. J Korean Acad Oral Maxillofac Radiol. 1992; 22:305–313.18. Lynch DC, Revil T, Schwartzentruber J, Bhoj EJ, Innes AM, Lamont RE, et al. Disrupted auto-regulation of the spliceosomal gene SNRPB causes cerebro-costo-mandibular syndrome. Nat Commun. 2014; 5:4483.
Article19. Bacrot S, Doyard M, Huber C, Alibeu O, Feldhahn N, Lehalle D, et al. Mutations in SNRPB, encoding components of the core splicing machinery, cause cerebro-costo-mandibular syndrome. Hum Mutat. 2015; 36:187–190.20. Cohen SM, Greathouse ST, Rabbani CC, O'Neil J, Kardatzke MA, Hall TE, et al. Robin sequence: what the multidisciplinary approach can do. J Multidiscip Healthc. 2017; 10:121–132.
Article21. Wagener S, Rayatt SS, Tatman AJ, Gornall P, Slator R. Management of infants with Pierre Robin sequence. Cleft Palate Craniofac J. 2003; 40:180–185.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Application of Temporary Tongue-Lip Traction During the Initial Period of Mandibular Distraction in Pierre Robin Sequence
- Surgical treatment of airway obstruction in infants with Pierre Robin sequence
- Tongue-lip adhesion in Pierre Robin sequence
- Management of a Dentigerous Cyst in a Child with Robin Sequence
- A Case of Pierre Robin Syndrome
