Alveolar ridge preservation with a collagen material: a randomized controlled trial
- Affiliations
-
- 1Private Practice, Hilzingen, Germany. info@schnutenhaus.de
- 2Department of Prosthetic Dentistry, Center of Dentistry, Ulm University, Ulm, Germany.
- 3Institute of Epidemiology and Medical Biometry, Ulm University, Ulm, Germany.
- KMID: 2465389
- DOI: http://doi.org/10.5051/jpis.2018.48.4.236
Abstract
- PURPOSE
Resorption of the alveolar bone is an unavoidable consequence of tooth extraction when appropriate alveolar ridge preservation (ARP) measures are not taken. The objective of this trial was to test the hypothesis that dimensional changes in the alveolar bone after tooth extraction would be reduced by inserting an equine collagen membrane and a collagen cone to fill and seal the alveolus (as ARP), in comparison to extraction with untreated alveoli.
METHODS
In this randomized clinical trial, 31 patients were directly treated with the collagen material after extraction of a tooth from the maxilla (the ARP group). Twenty-nine patients served as the control group. After extraction, no further treatment (i.e., no socket preservation measures) was performed in the control group. Changes in the alveolar process immediately after extraction and after an 8 (±1)-week healing period were evaluated 3-dimensionally. Blinded analyses were performed after superimposing the data from the digitalized impressions and surfaces generated by cone-beam computed tomography.
RESULTS
Both the ARP and control groups showed a reduction of bone in the alveolar area after tooth extraction. However, significantly less bone resorption was detected in the clinically relevant buccal region in the ARP group. The median bone reduction was 1.18 mm in the ARP group and 5.06 mm in the control group (P = 0.03).
CONCLUSIONS
The proposed hypothesis that inserting a combination material comprising a collagen cone and membrane would lead to a difference in alveolar bone preservation can be accepted for the clinically relevant buccal distance. In this area, implantation of the collagen material led to significantly less alveolar bone resorption. German Clinical Trials Register at www.drks.de, DRKS00004769.
Keyword
MeSH Terms
Figure
-

Figure 1 (A) Atraumatic tooth extraction with periotomes and forceps. (B) Introduction of the collagen cone with the membrane. (C) Temporary sutures to stabilize the combination material. (D) Status 3 months after implantation. (E) Impression of the alveolar cavity immediately after tooth extraction.
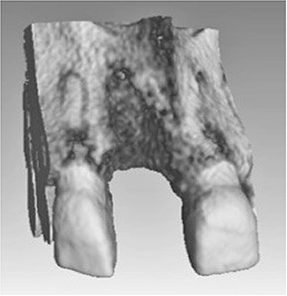
Figure 2 Cone-beam computed tomography image of the alveolus at 8 (±1) weeks after extraction.
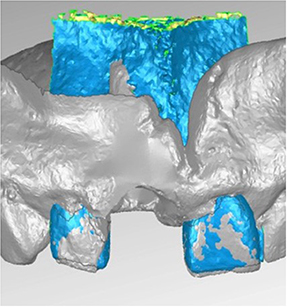
Figure 3 Matching of the models at time T0 and T1 via the hard tooth tissues.
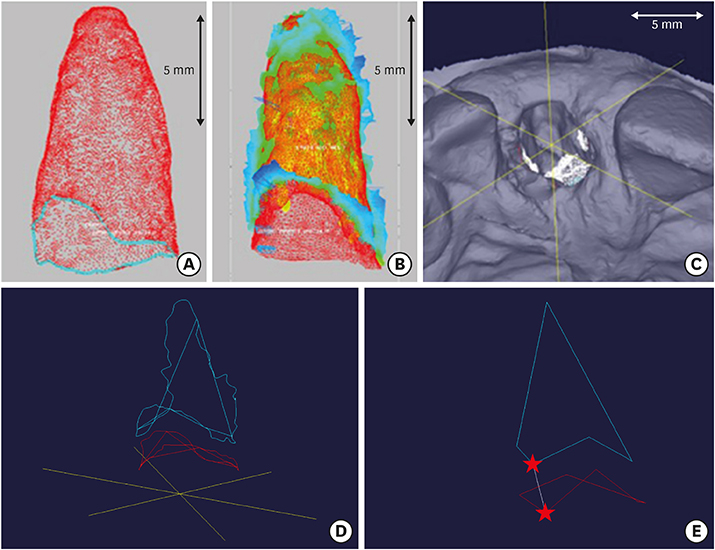
Figure 4 (A) Exposed surface of the post-extraction alveolus at time T0, immediately after tooth extraction. (B) Exposed surfaces from the impression at time T0 superimposed on the cone-beam computed tomography image (T1) at 8 (±1) weeks post extraction. (C) Specification of measurement points for the sextant measurements. (D) By using the intersections of the diagonal of the measuring aid and the 2 boundary curves, corner points were defined for the creation of 2 individual hexagons. (E) The distance of these constructed corner points was measured in the vertical direction. (★ to ★).
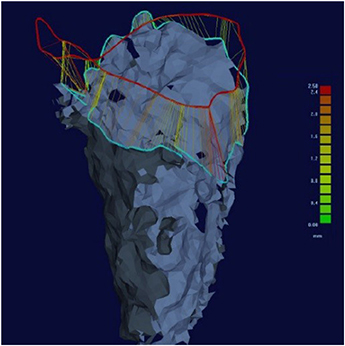
Figure 5 Three-dimensional measurements of the distances using boundary curves. Based on the 2 applied edge curves, the boundary curve difference was calculated. In each case, a lot was cut from the edge curve of alveolar impression at T0 on the edge curve of the cone-beam computed tomography image of the alveolus at T1. The resulting quantitative results provided the maximum deviation of 2 boundary curves, the mean, and the standard deviation.
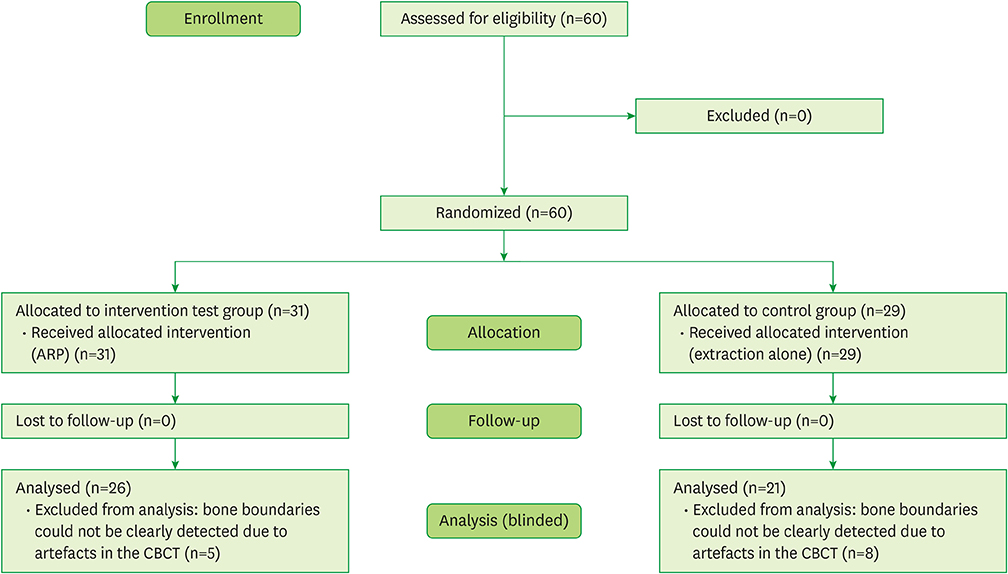
Figure 6 Flow diagram of this randomized trial comparing extraction alone to a ridge-preserving procedure for the treatment of alveolar bone after tooth removal. ARP: alveolar ridge preservation, CBCT: cone-beam computed tomography.

Figure 7 Significantly less bone degeneration was found along the buccal distance in the ARP group (mm). ARP: alveolar ridge preservation.
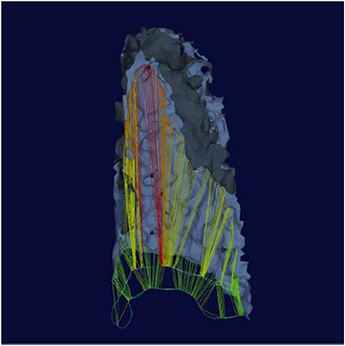
Figure 8 Almost complete destruction of the buccal bone was noted at 8 weeks after tooth extraction.
Reference
-
1. Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012; 23:Suppl 5. 1–21.
Article2. Chappuis V, Engel O, Reyes M, Shahim K, Nolte LP, Buser D. Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. J Dent Res. 2013; 92:195S–201S.3. Schmidlin PR, Jung RE, Schug J. Prevention of alveolar ridge resorption after tooth extraction--a review. Schweiz Monatsschr Zahnmed. 2004; 114:328–336.4. Iyer S, Haribabu PK, Xing Y. Part II. Minimizing alveolar bone loss during and after extractions. Protocol and techniques for alveolar bone preservation. Alpha Omegan. 2014; 107:14–25.5. Mardas N, Chadha V, Donos N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: a randomized, controlled clinical trial. Clin Oral Implants Res. 2010; 21:688–698.
Article6. Trombelli L, Farina R, Marzola A, Bozzi L, Liljenberg B, Lindhe J. Modeling and remodeling of human extraction sockets. J Clin Periodontol. 2008; 35:630–639.
Article7. Sanz I, Garcia-Gargallo M, Herrera D, Martin C, Figuero E, Sanz M. Surgical protocols for early implant placement in post-extraction sockets: a systematic review. Clin Oral Implants Res. 2012; 23:Suppl 5. 67–79.
Article8. Ten Heggeler JM, Slot DE, Van der Weijden GA. Effect of socket preservation therapies following tooth extraction in non-molar regions in humans: a systematic review. Clin Oral Implants Res. 2011; 22:779–788.
Article9. Misch CE, Dietsh-Misch F, Misch CM. A modified socket seal surgery with composite graft approach. J Oral Implantol. 1999; 25:244–250.
Article10. Crespi R, Capparè P, Gherlone EF. Bone recontouring in fresh sockets with buccal bone loss: a cone beam computed tomography study. Int J Oral Maxillofac Implants. 2014; 29:863–868.
Article11. Vittorini Orgeas G, Clementini M, De Risi V, de Sanctis M. Surgical techniques for alveolar socket preservation: a systematic review. Int J Oral Maxillofac Implants. 2013; 28:1049–1061.
Article12. Pagni G, Pellegrini G, Giannobile WV, Rasperini G. Postextraction alveolar ridge preservation: biological basis and treatments. Int J Dent. 2012; 2012:151030.
Article13. Lambert F, Vincent K, Vanhoutte V, Seidel L, Lecloux G, Rompen E. A methodological approach to assessing alveolar ridge preservation procedures in humans: hard tissue profile. J Clin Periodontol. 2012; 39:887–894.
Article14. Annen BM, Schneider D, Schmidlin PR. Ridge preservation after tooth extraction using collagen cones with integrated membranes: a case series and volumetric analysis. Implantologie. 2014; 22:341–351.15. Kunert-Keil C, Gredes T, Heinemann F, Dominiak M, Botzenhart U, Gedrange T. Socket augmentation using a commercial collagen-based product--an animal study in pigs. Mater Sci Eng C. 2015; 46:177–183.
Article16. Moher D, Schulz KF, Altman DG. CONSORT. The CONSORT statement: revised recommendations for improving the quality of reports of parallel group randomized trials. BMC Med Res Methodol. 2001; 1:2.
Article17. Schulz KF, Altman DG, Moher D. CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. 2010; 63:834–840.
Article18. Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, et al. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. 2010; 63:e1–e37.19. Fickl S, Zuhr O, Wachtel H, Stappert CF, Stein JM, Hürzeler MB. Dimensional changes of the alveolar ridge contour after different socket preservation techniques. J Clin Periodontol. 2008; 35:906–913.
Article20. de Avila ED, Filho JS, de Oliveira Ramalho LT, Real Gabrielli MF, Pereira Filho VA. Alveolar ridge augmentation with the perforated and nonperforated bone grafts. J Periodontal Implant Sci. 2014; 44:33–38.
Article21. Leung CC, Palomo L, Griffith R, Hans MG. Accuracy and reliability of cone-beam computed tomography for measuring alveolar bone height and detecting bony dehiscences and fenestrations. Am J Orthod Dentofacial Orthop. 2010; 137:S109–S119.
Article22. Schulze R, Heil U, Gross D, Bruellmann DD, Dranischnikow E, Schwanecke U, et al. Artefacts in CBCT: a review. Dentomaxillofac Radiol. 2011; 40:265–273.
Article23. Seibert JS, Cohen DW. Periodontal considerations in preparation for fixed and removable prosthodontics. Dent Clin North Am. 1987; 31:529–555.24. De Buitrago JG, Avila-Ortiz G, Elangovan S. Quality assessment of systematic reviews on alveolar ridge preservation. J Am Dent Assoc. 2013; 144:1349–1357.
Article25. Hämmerle CH, Araújo MG, Simion M. Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012; 23:Suppl 5. 80–82.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The study on ridge preservation for implant site development
- A clinico-radiographic and histomorphometric analysis of alveolar ridge preservation using calcium phosphosilicate, PRF, and collagen plug
- Improving oral rehabilitation through the preservation of the tissues through alveolar preservation
- Efficacy and safety of rhBMP/β-TCP in alveolar ridge preservation: a multicenter, randomized, open-label, comparative, investigator-blinded clinical trial
- Alveolar Ridge Preservation in the Severely Damaged Sockets of the Anterior Maxilla Followed by Delayed Implant Placement
