Significance of Sufficient Neck Flexion During Magnetic Resonance Imaging in the Diagnosis of Hirayama Disease: Report of Two Cases
- Affiliations
-
- 1Department of Rehabilitation Medicine, Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea. ripheonix@dsmc.or.kr
- 2Department of Physical and Rehabilitation Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2463708
- DOI: http://doi.org/10.5535/arm.2019.43.5.615
Abstract
- It is difficult to distinguish Hirayama disease (HD) from other mimicking disorders in adolescent patients with distal upper limb weakness. The prevailing theory of HD postulates that the lower cervical cord is susceptible to compression during neck flexion because of insufficient growth of the dura relative to the spinal column. Confirmation of a dynamic change in the dorsal epidural space on magnetic resonance imaging (MRI) during neck flexion is essential for diagnosing HD. However, neck flexion MRI has not been routinely performed in juvenile patients with distal upper limb weakness in the absence of suspected HD. We report two cases of HD that were initially confused with other diseases because of insufficient or absent cervical flexion during MRI. Full-flexion MRI showed typical findings of HD in both cases. Our cases suggest that dynamic cervical MRI in the fully flexed position is necessary for evaluating suspected HD.
MeSH Terms
Figure
-
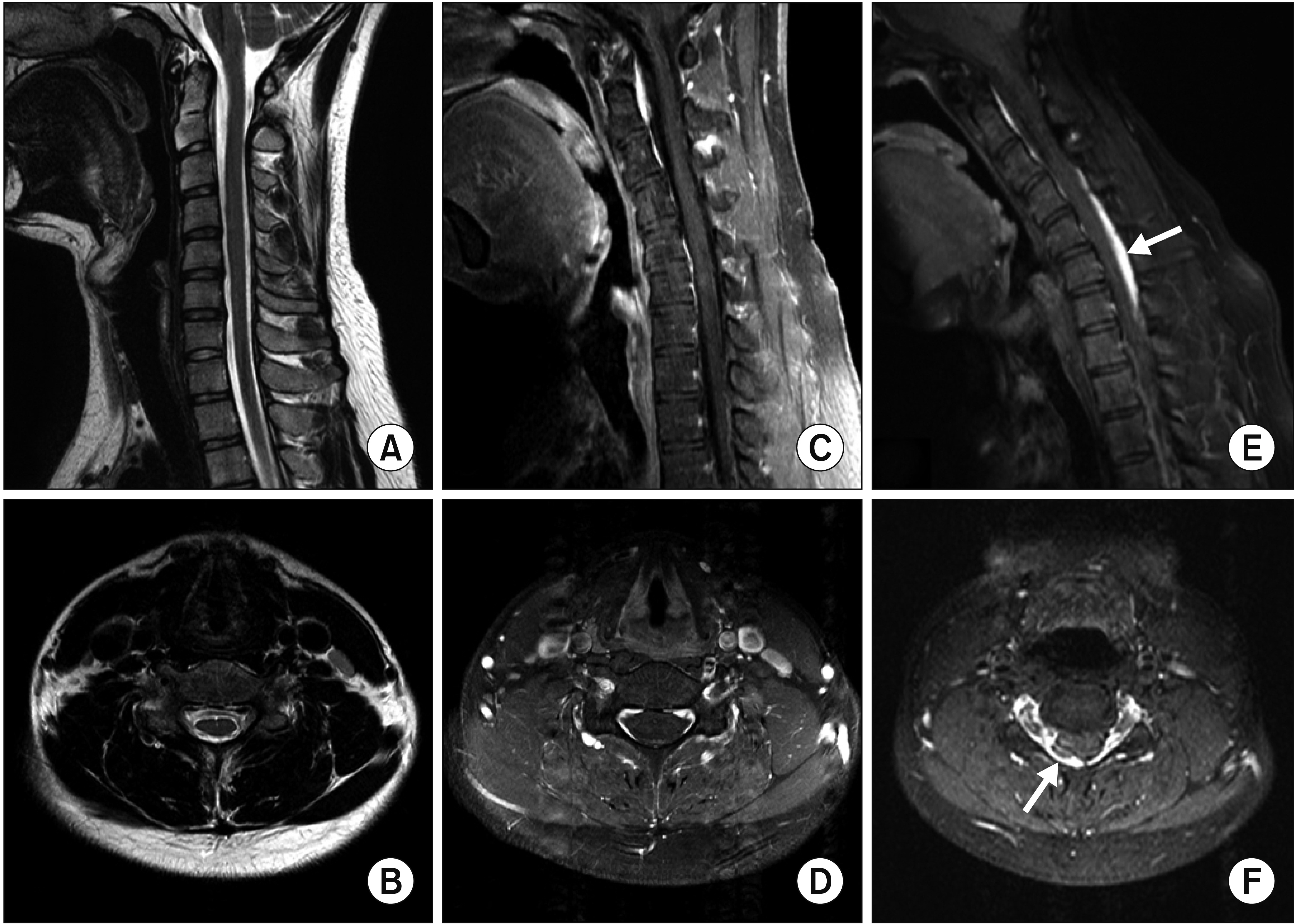
Fig. 1. (A, B) T2-weighted cervical magnetic resonance imaging (MRI) in the neutral position revealed no signal change or spinal cord atrophy. (C, D) Contrast-enhanced MRI in the suboptimal neck-flexion position did not show dural detachment from the adjacent lamina. (E) Sagittal contrast-enhanced MRI in the fully flexed position demonstrated a crescent-shaped enlarged posterior epidural space (arrow). (F) Axial contrast-enhanced MRI in the fully flexed position revealed right dural sac detachment from the lamina and spinal cord compression by the engorged posterior epidural venous plexus (arrow).
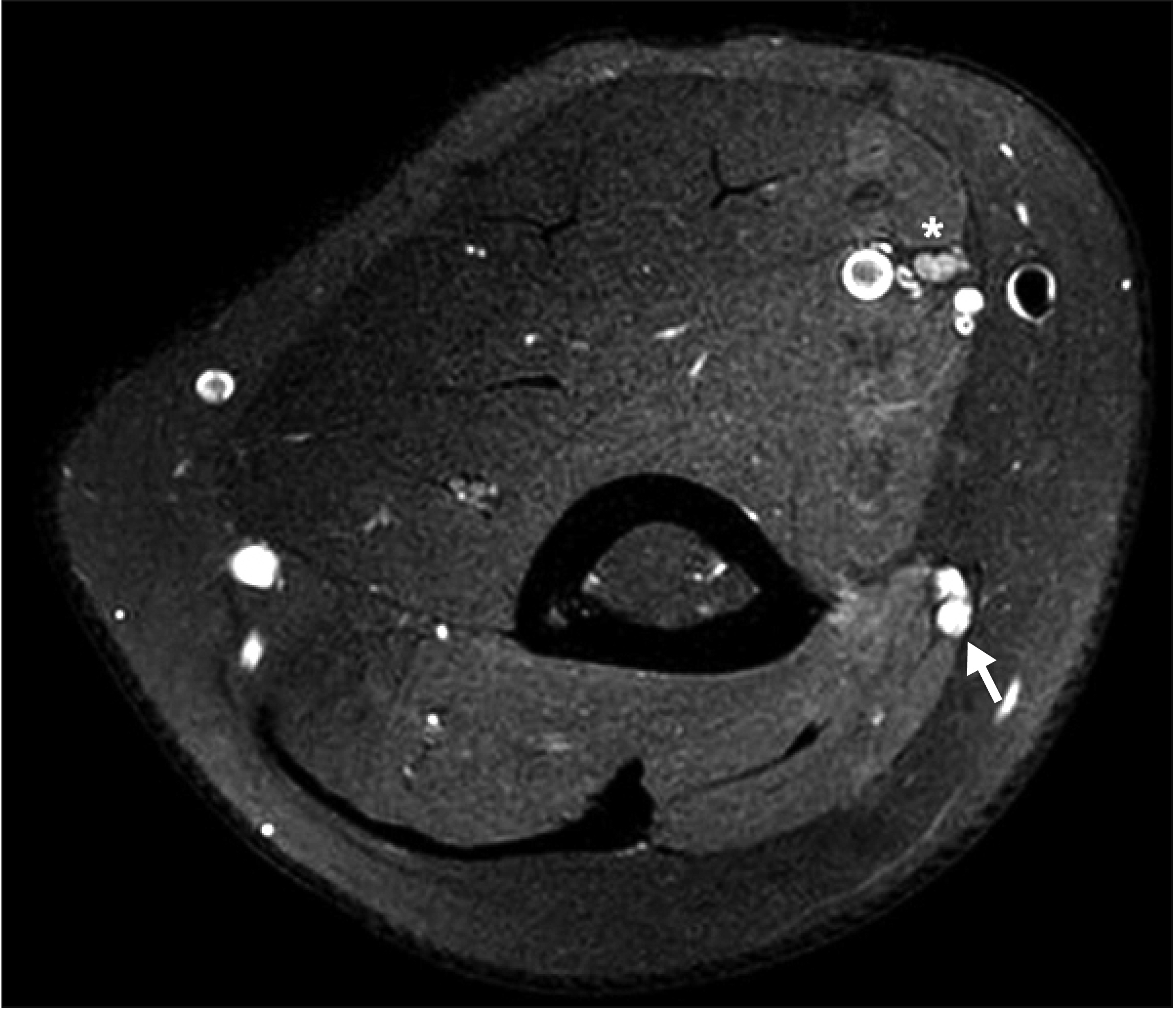
Fig. 2. Upper-arm magnetic resonance imaging revealed hyperintensity and swelling of the median (asterisk) and ulnar (arrow) nerves in the axial T2-weighted fat-suppressed turbo spin-echo sequence image.
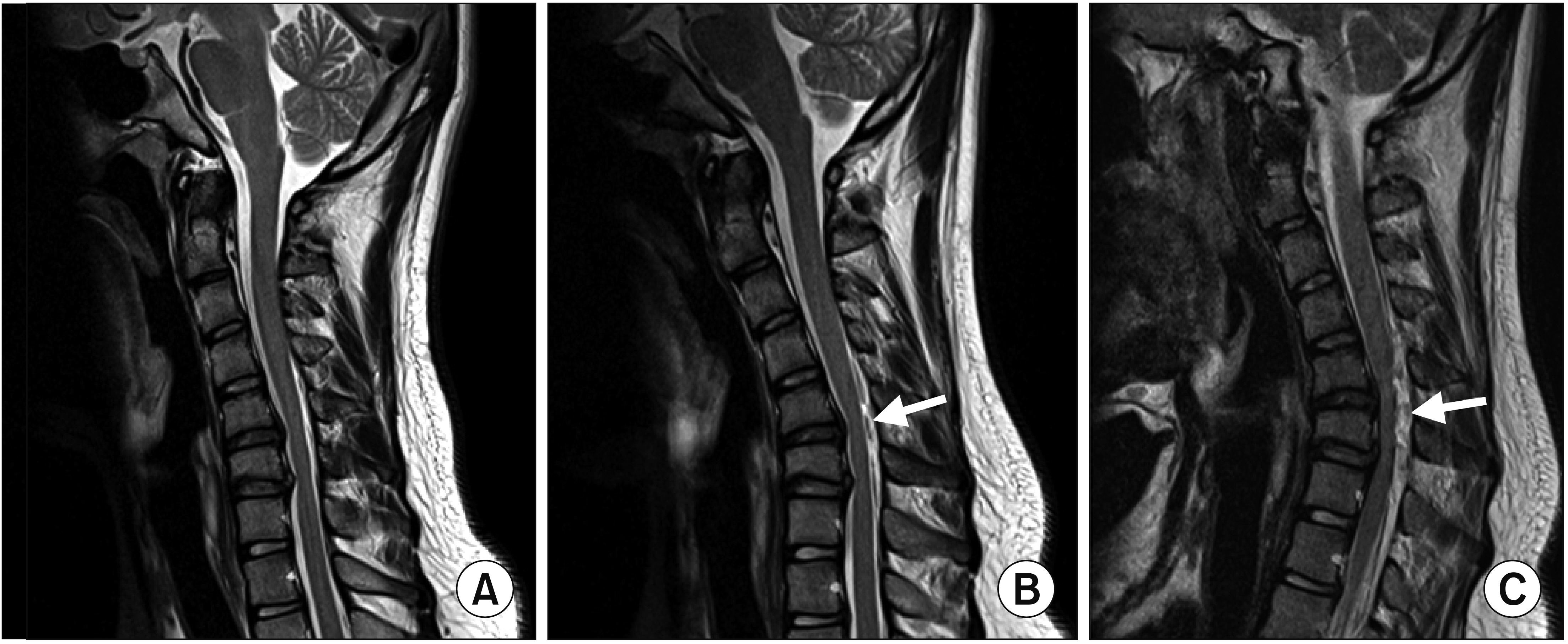
Fig. 3. (A) Cervical magnetic resonance imaging (MRI) in the neutral position showed disc protrusion at C5-6 and C6-7 in the sagittal T2-weighted image. (B) Cervical MRI with neck flexion revealed suspected dural detachment from the lamina (arrow). (C) Cervical MRI with full flexion demonstrated obvious widening of the dorsal epidural space with flattening of the cervical cord (arrow).
Reference
-
1. Schroder R, Keller E, Flacke S, Schmidt S, Pohl C, Klockgether T, et al. MRI findings in Hirayama’s disease: flexion-induced cervical myelopathy or intrinsic motor neuron disease? J Neurol. 1999; 246:1069–74.2. Tashiro K, Kikuchi S, Itoyama Y, Tokumaru Y, Sobue G, Mukai E, et al. Nationwide survey of juvenile muscular atrophy of distal upper extremity (Hirayama disease) in Japan. Amyotroph Lateral Scler. 2006; 7:38–45.
Article3. Hirayama K. Juvenile muscular atrophy of distal upper extremity (Hirayama disease). Intern Med. 2000; 39:283–90.
Article4. Yoo SD, Kim HS, Yun DH, Kim DH, Chon J, Lee SA, et al. Monomelic amyotrophy (Hirayama disease) with upper motor neuron signs: a case report. Ann Rehabil Med. 2015; 39:122–7.
Article5. Lehman VT, Luetmer PH, Sorenson EJ, Carter RE, Gupta V, Fletcher GP, et al. Cervical spine MR imaging findings of patients with Hirayama disease in North America: a multisite study. AJNR Am J Neuroradiol. 2013; 34:451–6.
Article6. Zhou B, Chen L, Fan D, Zhou D. Clinical features of Hirayama disease in mainland China. Amyotroph Lateral Scler. 2010; 11:133–9.
Article7. Hirayama K, Toyokura Y, Tsubaki T. Juvenile muscular atrophy of unilateral upper extremity: a new clinical entity. Psychiatr Neurol Jpn. 1959; 61:2190–8.8. Hou C, Han H, Yang X, Xu X, Gao H, Fan D, et al. How does the neck flexion affect the cervical MRI features of Hirayama disease? Neurol Sci. 2012; 33:1101–5.
Article9. Hirayama K, Tokumaru Y. Cervical dural sac and spinal cord in juvenile muscular atrophy of distal upper extremity. Neurology. 2000; 54:1922–6.
Article10. Lapresle J. Clinical and neuropathological aspects of circulatory disorders of the spinal cord. Bull Schweiz Akad Med Wiss. 1969; 24:512–28.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Experiences of Uncommon Motor Neuron Disease: Hirayama Disease
- Two Cases of Hirayama Disease in a Pediatric Clinic
- A Korean Case of Juvenile Muscular Atrophy of Distal Upper Extremity (Hirayama Disease) with Dynamic Cervical Cord Compression
- Hirayama Disease with Proximal Involvement
- Hirayama Disease with Isolated Spinal Cord Atrophy
