A Korean Case of Juvenile Muscular Atrophy of Distal Upper Extremity (Hirayama Disease) with Dynamic Cervical Cord Compression
- Affiliations
-
- 1Department of Neurology, Seoul National University Hospital, Seoul, Korea. kimmanho@snu.ac.kr
- 2Department of Neurology, Eulji General Hospital, Eulji University School of Medicine, Seoul, Korea.
- KMID: 1733526
- DOI: http://doi.org/10.3346/jkms.2004.19.5.768
Abstract
- We present a Korean case of Hirayama disease with its typical neuroradiological findings of forward displacement of cervical dural sac and compression of the lower cervical cord during neck flexion. A 15-yr-old boy was presented with a one-year history of progressive weakness and atrophy affecting bilateral hands and forearms. The electrodiagnostic findings were compatible with the lesion of the anterior horn cells at the C7, C8, and T1 spinal segments. With neck flexion, cervical magnetic resonance imaging (MRI) showed the anterior shifting of the lower cervical dural sac resulting in the cord compression of those segments. Presumably, this disease might have been prevalent in Korea frequently under the diagnosis of "benign focal amyotrophy". In this regard, we discuss the clinical importance of cervical MRI with neck flexion and anticipate the increasing reports of the case substantiated by its characteristic radiological features.
MeSH Terms
Figure
-

Fig. 1 T2-weighted sagittal images in the neutral position reveals normal contour and signal intensity along the sixth to the eighth cervical segments without cervical cord compression.

Fig. 2 (A) On T2-weighted sagittal images in the anteflexed position, there is an anterior shifting of the posterior wall of the cervical dural sac below the third cervical vertebral level compressing the cervical spinal cord from the fifth cervical to the first thoracic vertebral levels (row of white arrows). (B) On enhancement, the widened posterior epidural space shows a homogenous strong enhancement with some signal flow void, suggesting a passively widened epidural venous plexus.
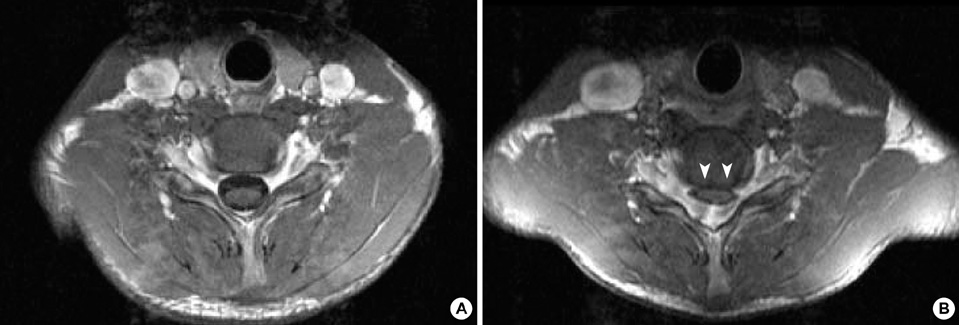
Fig. 3 (A) The T1-weighted axial image of the sixth cervical cord segment in the neutral position has a normal appearance. (B) There is a striking forward compression by the posterior dural sac in the enhanced axial image of the same cervical cord segment in the anteflexed position (white arrowheads).
Reference
-
1. Hirayama K, Toyokura Y, Tsubaki T. Juvenile muscular atrophy of unilateral upper extremity; a new clinical entity. Psychiatr Neurol Jpn. 1959. 61:2190–2197.2. Pradhan S, Gupta RK. Magnetic resonance imaging in juvenile asymmetric segmental spinal muscular atrophy. J Neurol Sci. 1997. 146:133–138.
Article3. Chen CJ, Chen CM, Wu CL, Ro LS, Chen ST, Lee TH. Hirayama disease: MR diagnosis. AJNR Am J Neuroradiol. 1998. 19:365–368.4. Choi IS. Two cases of juvenile muscular atrophy confined to upper limb. J Korean Med Assoc. 1982. 25:669–670.5. Choi IS. Benign focal amyotrophy. J Korean Med Assoc. 1987. 30:1371–1374.6. Cheong KH, Cho PZ, Sunwoo IN, Park YK, Lee SA, Kim KW, Park KD. Clinical characteristics of benign focal amyotrophy. Korean J Neurol. 1992. 10:447–456.7. Kim JY, Lee KW, Roh JK, Chi JG, Lee SB. A clinical study of benign focal amyotrophy. J Korean Med Sci. 1994. 9:145–154.
Article8. Hirayama K, Tokumaru Y. Cervical dural sac and spinal cord in juvenile muscular atrophy of distal upper extremity. Neurology. 2000. 54:1922–1926.
Article9. Kohno M, Takahashi H, Yagishita A, Tanabe H. "Disproportion theory" of the cervical spine and spinal cord in patients with juvenile cervical flexion myelopathy-a study comparing cervical magnetic resonance images with those of normal controls. Surg Neurol. 1998. 50:421–430.10. Hirayama K. Juvenile muscular atrophy of distal upper extremity (Hirayama disease): Focal cervical ischemic poliomyelopathy. Neuropathology. 2000. 20:S91–S94.
Article11. Toma S, Shiozawa Z. Amyotrophic cervical myelopathy in adolescence. J Neurol Neurosurg Psychiatry. 1995. 58:56–64.
Article12. Schroder R, Keller E, Flacke S, Schmidt S, Klockgether T, Schlegel U. MRI findings in Hirayama's disease: flexion-induced cervical myelopathy or intrinsic motor neuron disease? J Neurol. 1999. 246:1069–1074.13. Robberecht W, Aguirre T, Van Den Bosch L, Theys P, Nees H, Cassiman JJ, Matthijs G. Familial juvenile focal amyotrophy of the upper extremity (Hirayama disease): Superoxide dismutase 1 genotype and activity. Arch Neurol. 1997. 54:46–50.14. Saito M. Segmental muscular atrophy of distal upper extremity with juvenile onset. J Nagoya Med Assoc. 1977. 99:82–112.15. Gourie-Devi M, Suresh TG, Shankar SK. Monomelic amyotrophy. Arch Neurol. 1984. 41:388–394.
Article16. Adornato BT, Engle WK, Kucera J, Bertorini TE. Benign focal amyotrophy. Neurology. 1978. 28:399.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Experiences of Uncommon Motor Neuron Disease: Hirayama Disease
- Anterior Cervical Discectomy and Fusion for Hirayama Disease: a Case Report and Literature Review
- A Case of the Hirayama Disease in Young Male Adolescent
- MRI Findings of Nonprogressive Juvenile Spinal Muscular Atrophy of the Distal Upper Limbs (Hirayama's Disease)
- Monomelic Amyotrophy (Hirayama Disease) With Upper Motor Neuron Signs: A Case Report
