Correction of Spondylolisthesis by Lateral Lumbar Interbody Fusion Compared with Transforaminal Lumbar Interbody Fusion at L4–5
- Affiliations
-
- 1Department of Neurosurgery, Chung-Ang University Hospital, Seoul, Korea. nspsw@cau.ac.kr
- KMID: 2463673
- DOI: http://doi.org/10.3340/jkns.2018.0143
Abstract
OBJECTIVE
In an aging society, the number of patients with symptomatic degenerative spondylolisthesis (DS) is increasing and there is an emerging need for fusion surgery. However, few studies have compared transforaminal lumbar interbody fusion (TLIF) and lateral lumbar interbody fusion (LLIF) for the treatment of patients with DS. The purpose of this study was to investigate the clinical and radiological outcomes between TLIF and LLIF in DS.
METHODS
We enrolled patients with symptomatic DS at L4-5 who underwent TLIF with open pedicle screw fixation (TLIF group, n=41) or minimally invasive LLIF with percutaneous pedicle screw fixation (LLIF group, n=39) and were followed-up for more than one year. Clinical (visual analog scale and Oswestry disability index) and radiological outcomes (spondylolisthesis rate, segmental sagittal angle [SSA], mean disc height [MDH], intervertebral foramen height [FH], cage subsidence, and fusion rate) were assessed. And we assessed the changes in radiological parameters between the postoperative and the last follow-up periods.
RESULTS
Preoperative radiological parameters were not significantly different between the two groups. LLIF was significantly superior to TLIF in immediate postoperative radiological results, including reduction of spondylolisthesis rate (3.8% and 7.2%), increase in MDH (13.9 mm and 10.3 mm) and FH (21.9 mm and 19.4 mm), and correction of SSA (18.9° and 15.6°) (p<0.01), and the changes were more stable from the postoperative period to the last follow-up (p<0.01). Cage subsidence was observed significantly less in LLIF (n=6) than TLIF (n=21). Fusion rate was not different between the two groups. The clinical outcomes did not differ significantly at any time point between the two groups. Complications were not statistically significant. However, TLIF showed chronic mechanical problems with screw loosening in four patients and LLIF showed temporary symptoms associated with the surgical approach, such as psoas and ileus muscle symptoms in three and two cases, respectively.
CONCLUSION
LLIF was more effective than TLIF for spondylolisthesis reduction, likely due to the higher profile cage and ligamentotactic effect. In addition, LLIF showed mechanical stability of the reduction level by using a cage with a larger footprint. Therefore, LLIF should be considered a surgical option before TLIF for patients with unstable DS.
MeSH Terms
Figure
-
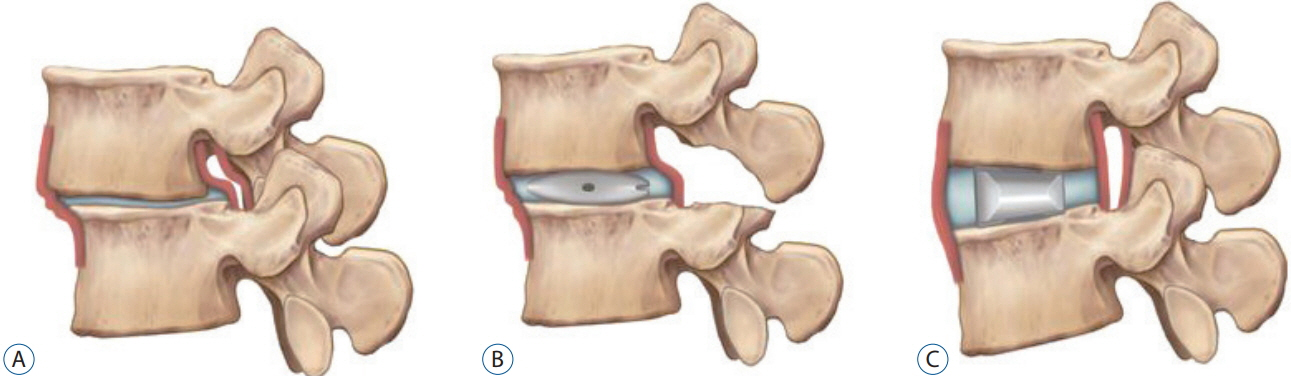
Fig. 1. Spondylolisthesis reduction in TLIF and LLIF. In preoperative state of DS, disc bulging and bucking of posterior longitudinal ligament and ligamentum flavum cause stenosis (A). TLIF improves stenosis through direct decompression of posterior elements, but it is difficult to insert of a cage with sufficient height, which is disadvantageous in terms of the spondylolisthesis reduction (B). LLIF can maximize the ligamentotaxic effect through insertion of cage with sufficient height, which indirectly decompresses the foraminal stenosis as well as corrects the DS effectively (C). TLIF : transforaminal lumbar interbody fusion, LLIF : lateral lumbar interbody fusion, DS : degenerative spondylolisthesis.
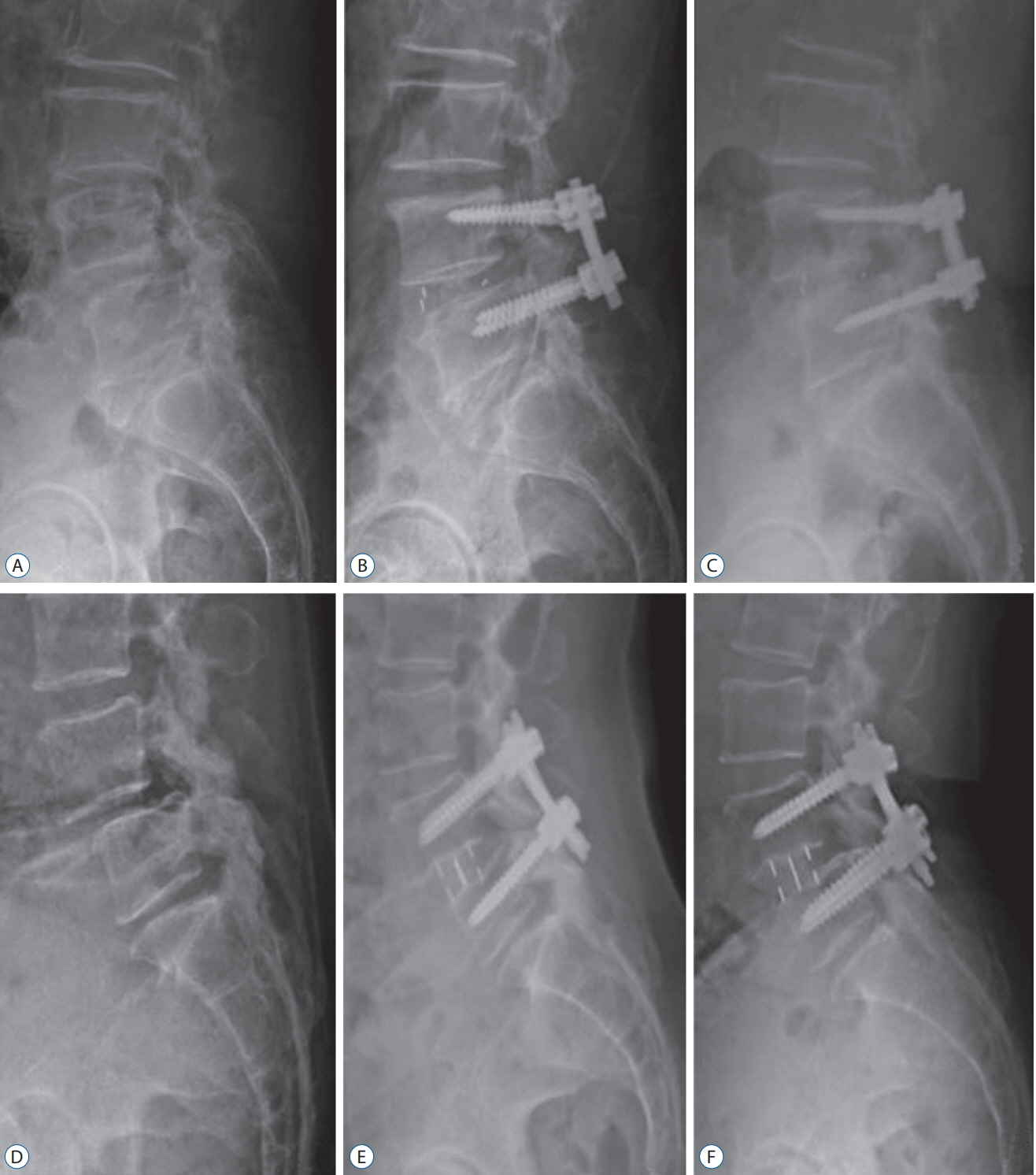
Fig. 2. Cases showing the largest change of reduced spondylolisthesis from immediate postoperative to last follow-up X-ray. In TLIF case, spondylolisthesis rate was 23.6% at preoperative (A), and reduced to 7.5% at immediately postoperative (B). It was slipped to 21.2% at 23 months after surgery (C). In LLIF case, spondylolisthesis rate was 28.7% at preoperative (D), and reduced to 6.7% at immediately postoperative (E). Then, it was 10.4% at 45 months after surgery (F). TLIF : transforaminal lumbar interbody fusion, LLIF : lateral lumbar interbody fusion.
Reference
-
References
1. Abdu WA, Sacks OA, Tosteson ANA, Zhao W, Tosteson TD, Morgan TS, et al. Long-term results of surgery compared with nonoperative treatment for lumbar degenerative spondylolisthesis in the spine patient outcomes research trial (SPORT). Spine (Phila Pa 1976). 43:1619–1630. 2018.
Article2. Ahlquist S, Park HY, Gatto J, Shamie AN, Park DY. Does approach matter? A comparative radiographic analysis of spinopelvic parameters in single-level lumbar fusion. Spine J. 18:1999–2008. 2018.
Article3. Anand N, Cohen RB, Cohen J, Kahndehroo B, Kahwaty S, Baron E. the influence of lordotic cages on creating sagittal balance in the CMIS treatment of adult spinal deformity. Int J Spine Surg. 11:23. 2017.
Article4. Bridwell KH, Lenke LG, McEnery KW, Baldus C, Blanke K. Anterior fresh frozen structural allografts in the thoracic and lumbar spine. Do they work if combined with posterior fusion and instrumentation in adult patients with kyphosis or anterior column defects? Spine (Phila Pa 1976). 20:1410–1418. 1995.
Article5. Campbell PG, Nunley PD, Cavanaugh D, Kerr E, Utter PA, Frank K, et al. Short-term outcomes of lateral lumbar interbody fusion without decompression for the treatment of symptomatic degenerative spondylolisthesis at L4-5. Neurosurg Focus. 44:E6. 2018.
Article6. Derman PB, Albert TJ. Interbody fusion techniques in the surgical management of degenerative lumbar spondylolisthesis. Curr Rev Musculoskelet Med. 10:530–538. 2017.
Article7. Elowitz EH. Central and foraminal indirect decompression in MIS lateral interbody fusion (XLIF): video lecture. Eur Spine J 24 Suppl. 3:449–450. 2015.
Article8. Foley KT, Holly LT, Schwender JD. Minimally invasive lumbar fusion. Spine (Phila Pa 1976). 28(15 Suppl):S26–S35. 2003.
Article9. Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge SN, et al. Laminectomy plus fusion versus laminectomy alone for lumbar spondylolisthesis. N Engl J Med. 374:1424–1434. 2016.
Article10. Goyal A, Kerezoudis P, Alvi MA, Goncalves S, Bydon M. Outcomes following minimally invasive lateral transpsoas interbody fusion for degenerative low grade lumbar spondylolisthesis: a systematic review. Clin Neurol Neurosurg. 167:122–128. 2018.
Article11. Guigui P, Ferrero E. Surgical treatment of degenerative spondylolisthesis. Orthop Traumatol Surg Res. 103(1S):S11–S20. 2017.
Article12. Harms J, Rolinger H. A one-stager procedure in operative treatment of spondylolistheses: dorsal traction-reposition and anterior fusion (author’s transl). Z Orthop Ihre Grenzgeb. 120:343–347. 1982.13. He LC, Wang YX, Gong JS, Griffith JF, Zeng XJ, Kwok AW, et al. Prevalence and risk factors of lumbar spondylolisthesis in elderly Chinese men and women. Eur Radiol. 24:441–448. 2014.
Article14. Hong TH, Cho KJ, Kim YT, Park JW, Seo BH, Kim NC. Does lordotic angle of cage determine lumbar lordosis in lumbar interbody fusion? Spine (Phila Pa 1976). 42:E775–E780. 2017.
Article15. Isaacs RE, Sembrano JN, Tohmeh AG; SOLAS Degenerative Study Group. Two-year comparative outcomes of MIS lateral and MIS transforaminal interbody fusion in the treatment of degenerative spondylolisthesis: Part II: radiographic findings. Spine (Phila Pa 1976) 41 Suppl. 8:S133–S144. 2016.16. Jacobsen S, Sonne-Holm S, Rovsing H, Monrad H, Gebuhr P. Degenerative lumbar spondylolisthesis: an epidemiological perspective: the Copenhagen osteoarthritis study. Spine (Phila Pa 1976). 32:120–125. 2007.17. Kuner EH, Kuner A, Schlickewei W, Mullaji AB. Ligamentotaxis with an internal spinal fixator for thoracolumbar fractures. J Bone Joint Surg Br. 76:107–112. 1994.
Article18. Lee CW, Yoon KJ, Ha SS. Which approach is advantageous to preventing development of adjacent segment disease? Comparative analysis of 3 different lumbar interbody fusion techniques (ALIF, LLIF, and PLIF) in L4-5 spondylolisthesis. World Neurosurg. 105:612–622. 2017.
Article19. Lee YS, Kim YB, Park SW, Chung C. Comparison of transforaminal lumbar interbody fusion with direct lumbar interbody fusion: clinical and radiological results. J Korean Neurosurg Soc. 56:469–474. 2014.
Article20. Melikian R, Yoon ST, Kim JY, Park KY, Yoon C, Hutton W. Sagittal plane correction using the lateral transpsoas approach: a biomechanical study on the effect of cage angle and surgical technique on segmental lordosis. Spine (Phila Pa 1976). 41:E1016–E1021. 2016.21. Min JH, Jang JS, Kim SK, Maeng DH, Lee SH. The ligamentotactic effect on a herniated disc at the level adjacent to the anterior lumbar interbody fusion : report of two cases. J Korean Neurosurg Soc. 46:65–67. 2009.
Article22. Pawar AY, Hughes AP, Sama AA, Girardi FP, Lebl DR, Cammisa FP. A comparative study of lateral lumbar interbody fusion and posterior lumbar interbody fusion in degenerative lumbar spondylolisthesis. Asian Spine J. 9:668–674. 2015.
Article23. Pereira EA, Farwana M, Lam KS. Extreme lateral interbody fusion relieves symptoms of spinal stenosis and low-grade spondylolisthesis by indirect decompression in complex patients. J Clin Neurosci. 35:56–61. 2017.
Article24. Resnick DK, Watters WC 3rd, Sharan A, Mummaneni PV, Dailey AT, Wang JC, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 9: lumbar fusion for stenosis with spondylolisthesis. J Neurosurg Spine. 21:54–61. 2014.
Article25. Sembrano JN, Tohmeh A, Isaacs R; SOLAS Degenerative Study Group. Two-year comparative outcomes of MIS lateral and MIS transforaminal interbody fusion in the treatment of degenerative spondylolisthesis: Part I: clinical findings. Spine (Phila Pa 1976) 41 Suppl. 8:S123–S132. 2016.26. Sembrano JN, Yson SC, Horazdovsky RD, Santos ER, Polly DW Jr. Radiographic comparison of lateral lumbar interbody fusion versus traditional fusion approaches: analysis of sagittal contour change. Int J Spine Surg. 9:16. 2015.
Article27. Tan GH, Goss BG, Thorpe PJ, Williams RP. CT-based classification of long spinal allograft fusion. Eur Spine J. 16:1875–1881. 2007.
Article28. Uribe JS, Harris JE, Beckman JM, Turner AW, Mundis GM, Akbarnia BA. Finite element analysis of lordosis restoration with anterior longitudinal ligament release and lateral hyperlordotic cage placement. Eur Spine J 24 Suppl. 3:420–426. 2015.
Article29. Wáng YX, Deng M, Griffith JF, Kwok AW, Leung JC, Ahuja AT, et al. Lumbar spondylolisthesis progression and de novo spondylolisthesis in elderly Chinese men and women: a year-4 follow-up study. Spine (Phila Pa 1976). 41:1096–1103. 2016.
Article30. Xu DS, Bach K, Uribe JS. Minimally invasive anterior and lateral transpsoas approaches for closed reduction of grade II spondylolisthesis: initial clinical and radiographic experience. Neurosurg Focus. 44:E4. 2018.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Lateral Lumbar Interbody Fusion: Indications, Outcomes and Complications
- Uniportal Endoscopic Lumbar Interbody Fusion
- Lateral Lumbar Interbody Fusion
- Evaluation of Posterior Lumbar Interbody Fusion
- Morphometric Analysis of the Ureter with Respect to Lateral Lumbar Interbody Fusion Using Contrast-Enhanced Computed Tomography
