Value of Exhaled Nitric Oxide and FEF(25–75) in Identifying Factors Associated With Chronic Cough in Allergic Rhinitis
- Affiliations
-
- 1Department of Respiratory Medicine, Beijing Tongren Hospital, Capital Medical University, Beijing, China. suny@bjmu.edu.cn
- 2Department of Otolaryngology Head and Neck Surgery, Beijing Tongren Hospital, Capital Medical University, Beijing, China. dr.luozhang@139.com
- 3Key Laboratory of Otolaryngology Head and Neck Surgery of Ministry of Education of China, Beijing Institute of Otolaryngology, Beijing, China.
- 4Department of Respiratory Medicine, Peking University Third Hospital, Beijing, China.
- KMID: 2459187
- DOI: http://doi.org/10.4168/aair.2019.11.6.830
Abstract
- PURPOSE
Chronic cough in allergic rhinitis (AR) patients is common with multiple etiologies including cough variant asthma (CVA), non-asthmatic eosinophilic bronchitis (NAEB), gastroesophageal reflux-related cough (GERC), and upper airway cough syndrome (UACS). Practical indicators that distinguish these categories are lacking. We aimed to explore the diagnostic value of the fraction of exhaled nitric oxide (FeNO) and forced expiratory flow at 25% and 75% of pulmonary volume (FEF(25-75)) in specifically identifying CVA and NAEB in these patients.
METHODS
Consecutive AR patients with chronic cough were screened and underwent induced sputum, FeNO, nasal nitric oxide, spirometry, and methacholine bronchial provocation testing. All patients also completed gastroesophageal reflux disease questionnaires.
RESULTS
Among 1,680 AR patients, 324 (19.3%) were identified with chronic cough, of whom 316 (97.5%) underwent etiology analyses. Overall, 87 (27.5%) patients had chronic cough caused by NAEB, 78 (24.7%) by CVA, 16 (5.1%) by GERC, and 81 (25.6%) by UACS. Patients with either NAEB or CVA (n = 165, in total) were further assigned to a common group designated as CVA/NAEB, because they both responded to corticosteroid therapy. Receiver operating characteristic curves of FeNO revealed obvious differences among CVA, NAEB, and CVA/NAEB (area under the curve = 0.855, 0.699, and 0.923, respectively). The cutoff values of FeNO at 43.5 and 32.5 ppb were shown to best differentiate CVA and CVA/NAEB, respectively. FEF(25-75) was significantly lower in patients with CVA than in those with other causes. A FEF(25-75) value of 74.6% showed good sensitivity and specificity for identifying patients with CVA.
CONCLUSIONS
NAEB, CVA, and UACS are common causes of chronic cough in patients with AR. FeNO can first be used to discriminate patients with CVA/NAEB, then FEF(25-75) (or combined with FeNO) can further discriminate patients with CVA from those with CVA/NAEB.
Keyword
MeSH Terms
Figure
-
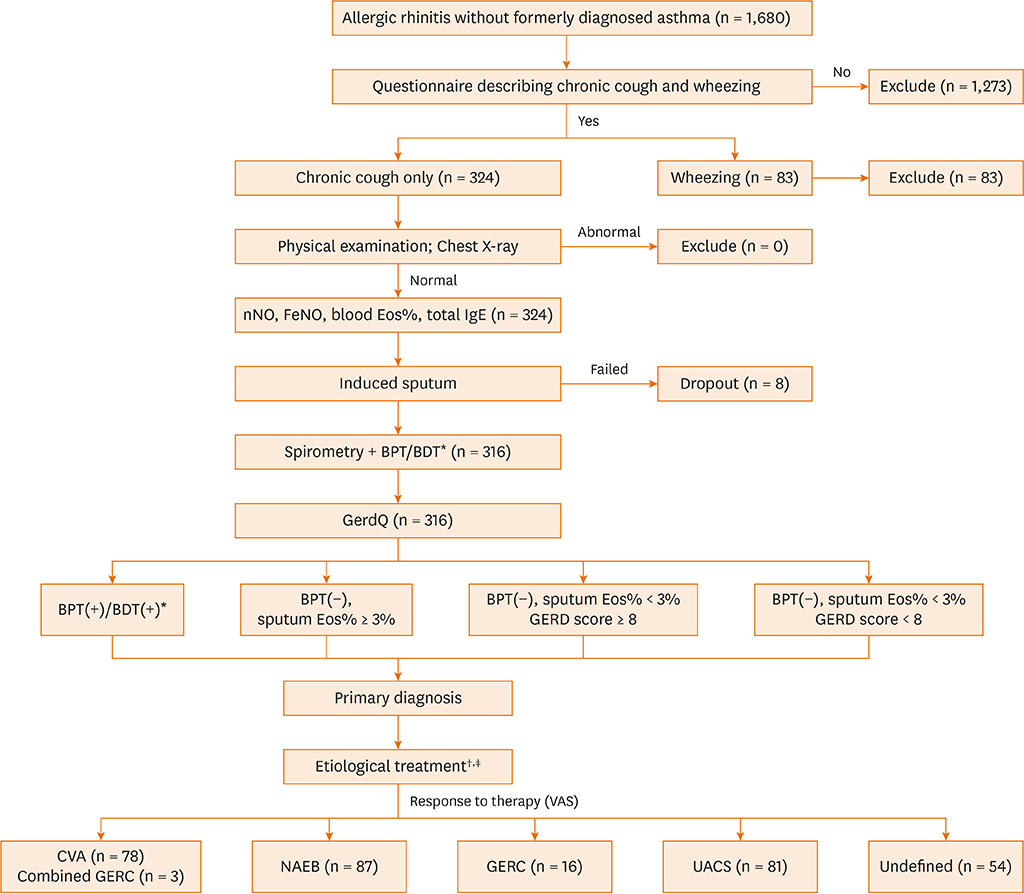
Fig. 1 Schematic diagram of the screening and diagnostic protocol used for chronic cough in AR patients. AR, allergic rhinitis; BDT, bronchial dilation test; BPT, bronchial provocation test; CVA, cough variant asthma; Eos, Eosinophils; FEF25–75: forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; GERC, gastroesophageal reflux-related cough; GERD, gastroesophageal reflux disease; GerdQ, gastroesophageal reflux disease questionnaire; ICS, inhaled corticosteroids; INCS, intranasal corticosteroids; LABA, long-acting beta2-agonist; NAEB, non-asthmatic eosinophilic bronchitis; nNO, nasal nitric oxide; PPI, proton pump inhibitor; UACS, upper airway cough syndrome; VAS, visual analogue scales; IgE, immunoglobulin E. *If FEV1 ≥ 70% predicted value, then conducted BPT; otherwise conducted BDT. †Etiological treatment: CVA, ICS plus bronchodilators (budesonide/formoterol, 320/9 µg bid 4 weeks, then reduced to 160/4.5 µg bid for at least 4 weeks at the relief of symptoms); NAEB, ICS (budesonide, 400 mg bid for 8 weeks); GERC, 1) lifestyle modification (losing weight; avoiding snacks at night, acidic drink, coffee, alcohol, chocolate, oily foods, and so forth) and 2) PPI (omeprazole, 20 mg bid). All the above treatments continued for at least 12 weeks; UACS, INCS (budesonide, 128 mg bid for 12 weeks) and second-generation antihistamine po (loratadine, 10 mg daily for 4 weeks). ‡Besides the etiological treatment for CVA, NAEB, GERC and the managements for GERC, all chronic cough patients received targeted therapy for AR.
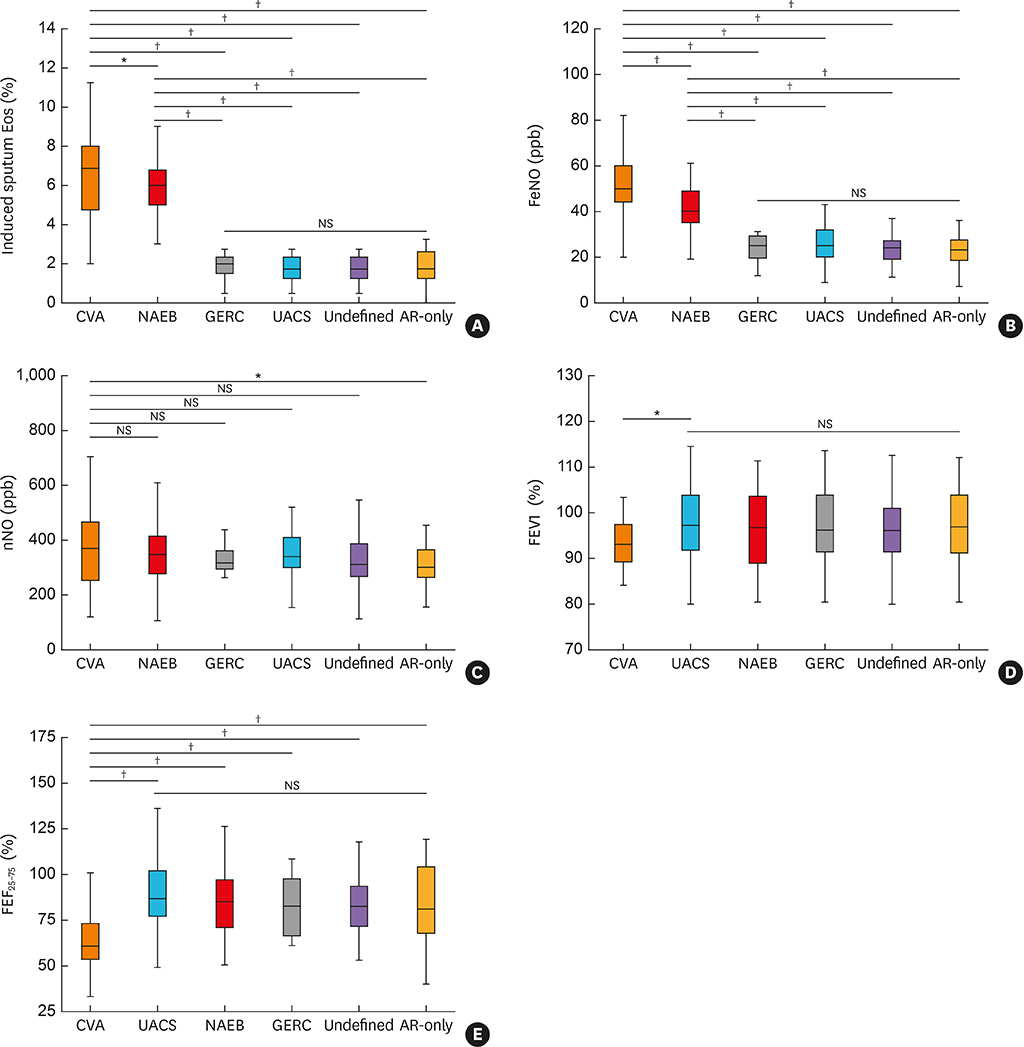
Fig. 2 Comparisons of induced sputum Eos (%) (A), FeNO (ppb) (B), nNO (ppb) (C), FEV1 (D), and FEF25–75 (E) among the different groups. NS, not significant; AR-only, allergic rhinitis patients without chronic cough; CVA, cough variant asthma; Eos, Eosinophils; FEF25–75, forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; GERC, gastroesophageal reflux-related cough; NAEB, non-asthmatic eosinophilic bronchitis; UACS, upper airway cough syndrome; nNO, nasal nitric oxide. *Statistical significance at P < 0.05; †Statistical significance at P < 0.01.
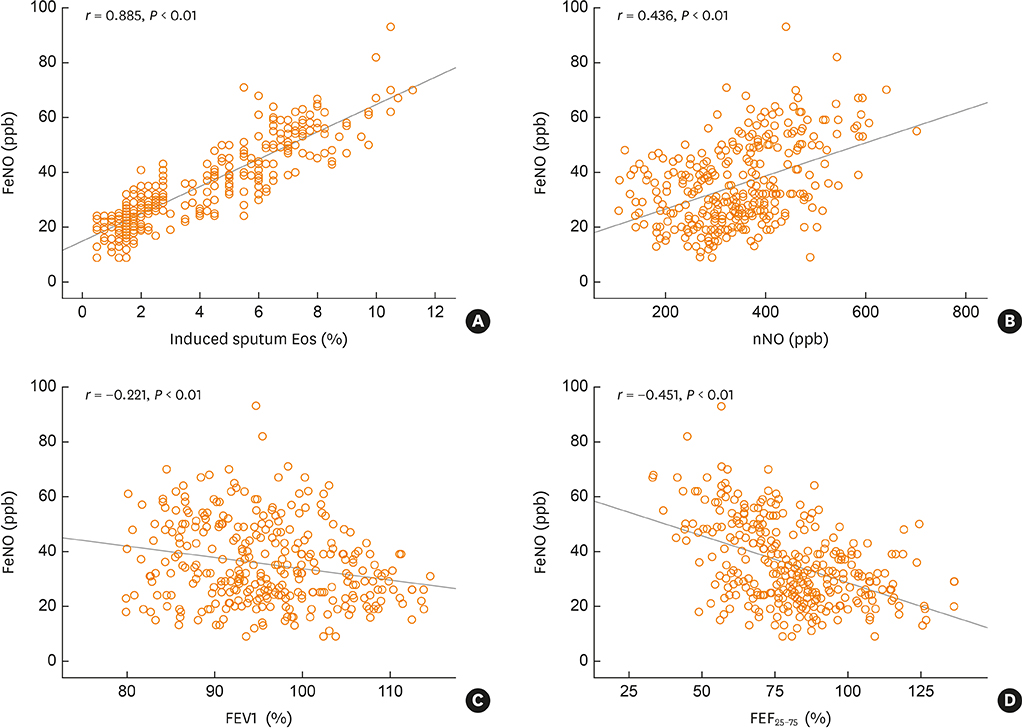
Fig. 3 Correlation of FeNO (ppb) with induced sputum Eos (%) (A), nNO (ppb) (B), FEV1 (C), and FEF25–75 (D). Pearson correlation coefficients were used for expressing the correlations. Eos, Eosinophils; FEF25–75: forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; nNO, nasal nitric oxide.
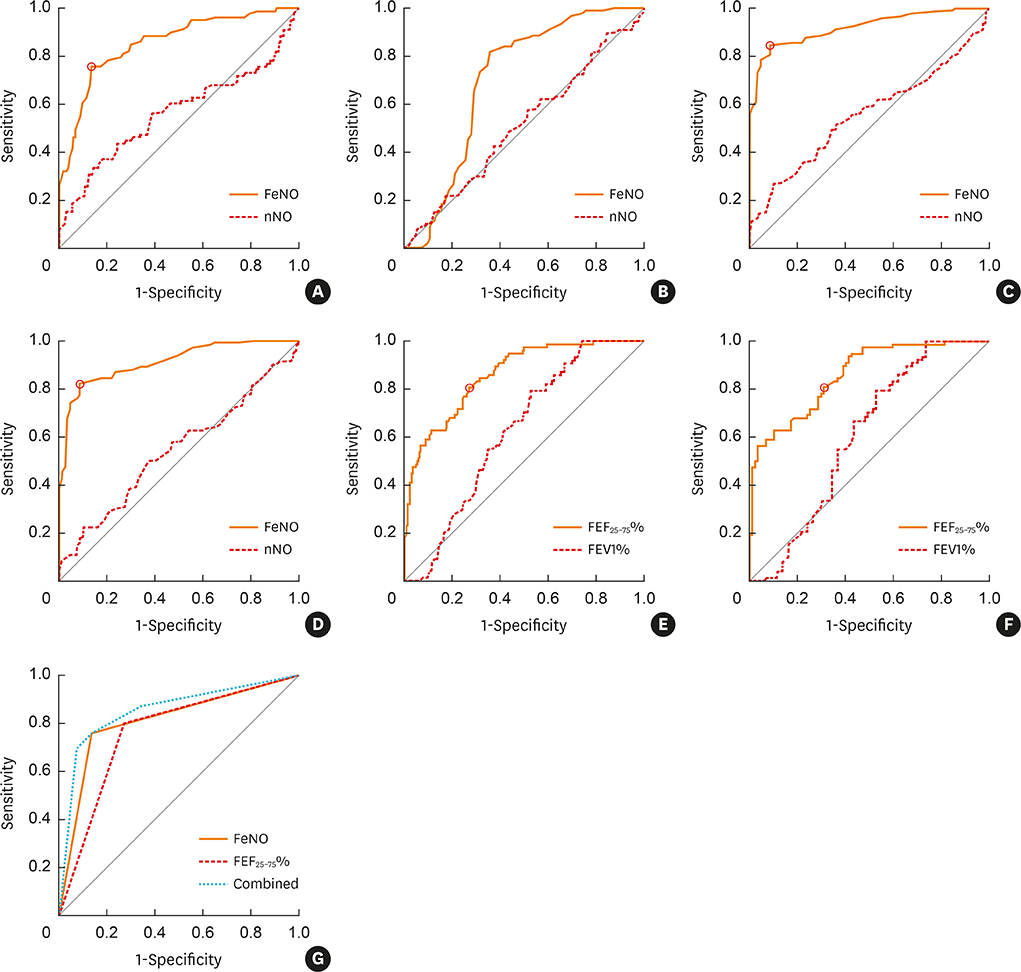
Fig. 4 ROC curves of FeNO, nNO, FEV1, and FEF25–75 for assessing diagnostic accuracy. ROC curves of FeNO and nNO for assessing the diagnostic accuracy for CVA (A), NAEB (B), CVA/NAEB (C), ROC curves of FeNO and nNO for assessing the diagnostic accuracy for NAEB in chronic cough without CVA (D), FEV1 and FEF25–75 for assessing the diagnostic accuracy for CVA in all chronic cough patients (E), for CVA only in CVA/NAEB patients (F), and FeNO model, FEF25–75 model, and combined model for assessing the diagnostic accuracy for CVA (G). ROC, receiver operating characteristic; CVA, cough variant asthma; CVA/NAEB, either NAEB or CVA; FEF25–75, forced expiratory flow at 25% and 75% of pulmonary volume; FeNO, fraction of exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; NAEB, non-asthmatic eosinophilic bronchitis; nNO, nasal nitric oxide.
Reference
-
1. Song WJ, Chang YS, Faruqi S, Kim JY, Kang MG, Kim S, et al. The global epidemiology of chronic cough in adults: a systematic review and meta-analysis. Eur Respir J. 2015; 45:1479–1481.
Article2. Iyer VN, Lim KG. Chronic cough: an update. Mayo Clin Proc. 2013; 88:1115–1126.
Article3. Irwin RS, French CL, Chang AB, Altman KW. CHEST Expert Cough Panel*. Classification of cough as a symptom in adults and management algorithms: CHEST guideline and expert panel report. Chest. 2018; 153:196–209.4. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008; 63:Suppl 86. 8–160.5. Katelaris CH, Lee BW, Potter PC, Maspero JF, Cingi C, Lopatin A, et al. Prevalence and diversity of allergic rhinitis in regions of the world beyond Europe and North America. Clin Exp Allergy. 2012; 42:186–207.
Article6. Meltzer EO. Allergic rhinitis: burden of illness, quality of life, comorbidities, and control. Immunol Allergy Clin North Am. 2016; 36:235–248.7. Hong Q, Bai C, Wang X. Characteristics of Chinese patients with cough in primary care centre. J Transl Med. 2011; 9:149.
Article8. Cho SH, Lin HC, Ghoshal AG, Bin Abdul Muttalif AR, Thanaviratananich S, Bagga S, et al. Respiratory disease in the Asia-Pacific region: cough as a key symptom. Allergy Asthma Proc. 2016; 37:131–140.
Article9. Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome): ACCP evidence-based clinical practice guidelines. Chest. 2006; 129:63S–71S.10. Tajiri T, Niimi A, Matsumoto H, Ito I, Oguma T, Otsuka K, et al. Prevalence and clinical relevance of allergic rhinitis in patients with classic asthma and cough variant asthma. Respiration. 2014; 87:211–218.
Article11. Lai K, Liu B, Xu D, Han L, Lin L, Xi Y, et al. Will nonasthmatic eosinophilic bronchitis develop into chronic airway obstruction?: a prospective, observational study. Chest. 2015; 148:887–894.12. Wang Z, Pianosi P, Keogh K, Zaiem F, Alsawas M, Alahdab F, et al. The clinical utility of fractional exhaled nitric oxide (FeNO) in asthma management. Rockville (MD): Agency for Healthcare Research and Quality;2017.13. Ciprandi G, Gallo F, Ricciardolo FL, Cirillo I. Fractional exhaled nitric oxide: a potential biomarker in allergic rhinitis? Int Arch Allergy Immunol. 2017; 172:99–105.
Article14. Krantz C, Janson C, Borres MP, Nordvall L, Alving K, Malinovschi A. Nasal nitric oxide is associated with exhaled NO, bronchial responsiveness and poor asthma control. J Breath Res. 2014; 8:026002.
Article15. Sato S, Saito J, Sato Y, Ishii T, Xintao W, Tanino Y, et al. Clinical usefulness of fractional exhaled nitric oxide for diagnosing prolonged cough. Respir Med. 2008; 102:1452–1459.
Article16. Maniscalco M, Faraone S, Sofia M, Molino A, Vatrella A, Zedda A. Extended analysis of exhaled and nasal nitric oxide for the evaluation of chronic cough. Respir Med. 2015; 109:970–974.
Article17. Bommarito L, Migliore E, Bugiani M, Heffler E, Guida G, Bucca C, et al. Exhaled nitric oxide in a population sample of adults. Respiration. 2008; 75:386–392.
Article18. Linhares D, Jacinto T, Pereira AM, Fonseca JA. Effects of atopy and rhinitis on exhaled nitric oxide values - a systematic review. Clin Transl Allergy. 2011; 1:8.
Article19. Dicpinigaitis PV. Chronic cough due to asthma: ACCP evidence-based clinical practice guidelines. Chest. 2006; 129:75S–79S.20. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of lung function testing: the authors' replies to readers' comments. Eur Respir J. 2010; 36:1496–1498.
Article21. Burgel PR. The role of small airways in obstructive airway diseases. Eur Respir Rev. 2011; 20:23–33.
Article22. Ciprandi G, Tosca MA, Signori A, Cirillo I. Bronchial hyperreactivity in patients with allergic rhinitis: forced expiratory flow between 25 and 75% of vital capacity might be a predictive factor. Allergy Asthma Proc. 2011; 32:4–8.
Article23. Ciprandi G, Tosca MA, Castellazzi AM, Cairello F, Salpietro C, Arrigo T, et al. FEF(25–75) might be a predictive factor for bronchial inflammation and bronchial hyperreactivity in adolescents with allergic rhinitis. Int J Immunopathol Pharmacol. 2011; 24:17–20.
Article24. Sposato B, Scalese M, Migliorini MG, Di Tomassi M, Scala R. Small airway impairment and bronchial hyperresponsiveness in asthma onset. Allergy Asthma Immunol Res. 2014; 6:242–251.
Article25. Morice AH, Fontana GA, Belvisi MG, Birring SS, Chung KF, Dicpinigaitis PV, et al. ERS guidelines on the assessment of cough. Eur Respir J. 2007; 29:1256–1276.
Article26. Kanemitsu Y, Matsumoto H, Oguma T, Nagasaki T, Ito I, Izuhara Y, et al. Independent factors contributing to daytime and nighttime asthmatic cough refractory to inhaled corticosteroids. J Investig Allergol Clin Immunol. 2019; 29:30–39.
Article27. Good JT Jr, Rollins DR, Kolakowski CA, Stevens AD, Denson JL, Martin RJ. New insights in the diagnosis of chronic refractory cough. Respir Med. 2018; 141:103–110.
Article28. Dreborg S. Skin testing. The safety of skin tests and the information obtained from using different methods and concentrations of allergen. Allergy. 1993; 48:473–475.29. American Thoracic Society. European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005; 171:912–930.30. Sohn SW, Lee HS, Park HW, Chang YS, Kim YK, Cho SH, et al. Evaluation of cytokine mRNA in induced sputum from patients with allergic rhinitis: relationship to airway hyperresponsiveness. Allergy. 2008; 63:268–273.31. Birnbaum S, Barreiro TJ. Methacholine challenge testing: identifying its diagnostic role, testing, coding, and reimbursement. Chest. 2007; 131:1932–1935.32. Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983; 148:839–843.
Article33. Lai K, Chen R, Lin J, Huang K, Shen H, Kong L, et al. A prospective, multicenter survey on causes of chronic cough in China. Chest. 2013; 143:613–620.
Article34. Mims JW. Asthma: definitions and pathophysiology. Int Forum Allergy Rhinol. 2015; 5:Suppl 1. S2–S6.
Article35. Yi F, Chen R, Luo W, Xu D, Han L, Liu B, et al. Validity of fractional exhaled nitric oxide in diagnosis of corticosteroid-responsive cough. Chest. 2016; 149:1042–1051.
Article36. Westerhof GA, Korevaar DA, Amelink M, de Nijs SB, de Groot JC, Wang J, et al. Biomarkers to identify sputum eosinophilia in different adult asthma phenotypes. Eur Respir J. 2015; 46:688–696.
Article37. Tang W, Zhou J, Miao L, Shi G. Clinical features in patients of cough variant asthma with normal and high level of exhaled fractional nitric oxide. Clin Respir J. 2018; 12:595–600.
Article38. Oh MJ, Lee JY, Lee BJ, Choi DC. Exhaled nitric oxide measurement is useful for the exclusion of nonasthmatic eosinophilic bronchitis in patients with chronic cough. Chest. 2008; 134:990–995.
Article39. Song WJ, Kim HJ, Shim JS, Won HK, Kang SY, Sohn KH, et al. Diagnostic accuracy of fractional exhaled nitric oxide measurement in predicting cough-variant asthma and eosinophilic bronchitis in adults with chronic cough: a systematic review and meta-analysis. J Allergy Clin Immunol. 2017; 140:701–709.40. Song DJ, Song WJ, Kwon JW, Kim GW, Kim MA, Kim MY, et al. KAAACI evidence-based clinical practice guidelines for chronic cough in adults and children in Korea. Allergy Asthma Immunol Res. 2018; 10:591–613.
Article41. Hsu JY, Wang CY, Cheng YW, Chou MC. Optimal value of fractional exhaled nitric oxide in inhaled corticosteroid treatment for patients with chronic cough of unknown cause. J Chin Med Assoc. 2013; 76:15–19.
Article42. Bao W, Zhang X, Lv C, Bao L, Yin J, Huang Z, et al. The value of fractional exhaled nitric oxide and forced mid-expiratory flow as predictive markers of bronchial hyperresponsiveness in adults with chronic cough. J Allergy Clin Immunol Pract. 2018; 6:1313–1320.
Article43. Muñoz-López F, Ríos-Alcolea M. The interest of FEF(25–75) in evaluating bronchial hyperresponsiveness with the methacholine test. Allergol Immunopathol (Madr). 2012; 40:352–356.
Article44. Niimi A. Cough associated with gastro-oesophageal reflux disease (GORD): Japanese experience. Pulm Pharmacol Ther. 2017; 47:59–65.
Article45. Kahrilas PJ, Altman KW, Chang AB, Field SK, Harding SM, Lane AP, et al. Chronic cough due to gastroesophageal reflux in adults: CHEST guideline and expert panel report. Chest. 2016; 150:1341–1360.46. Hulme K, Deary V, Dogan S, Parker SM. Psychological profile of individuals presenting with chronic cough. ERJ Open Res. 2017; 3:00099-2016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nasal and Exhaled Nitric Oxide in Allergic Rhinitis
- Clinical application of fractional exhaled nitric oxide in pediatric allergic rhinitis
- Exhaled nitric oxide and bronchial hyperresponsiveness in atopic asthmatic children with and without allergic rhinitis
- Fractional exhaled nitric oxide and forced expiratory volume in 1 second/forced vital capacity have predictive value of asthma exacerbation in Korean school children
- Exhaled NO: Determinants and Clinical Application in Children With Allergic Airway Disease
