Prevalence, Characteristics, and Clinical Significance of Concomitant Cardiomyopathies in Subjects with Bicuspid Aortic Valves
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Myongji Hospital, Hanyang University College of Medicine, Goyang, Korea.
- 2Division of Cardiology, Department of Internal Medicine, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. cysprs@yuhs.ac
- 3Department of Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Cardiology, Department of Internal Medicine, Sejong General Hospital, Bucheon, Korea.
- KMID: 2457477
- DOI: http://doi.org/10.3349/ymj.2019.60.9.816
Abstract
- PURPOSE
The present study aimed to investigate the prevalence, characteristics, and clinical significance of concomitant specific cardiomyopathies in subjects with bicuspid aortic valves (BAVs).
MATERIALS AND METHODS
A total of 1186 adults with BAV (850 males, mean age 56±14 years) at a single tertiary center were comprehensively reviewed. Left ventricular non-compaction, hypertrophic cardiomyopathy, and idiopathic dilated cardiomyopathy were confirmed when patients fulfilled current clinical and echocardiographic criteria. Clinical and echocardiographic characteristics, including comorbidities, heart failure presentation, BAV morphology, function, and aorta phenotypes, in BAV subjects with or without specific cardiomyopathies were compared.
RESULTS
Overall, 67 subjects (5.6%) had concomitant cardiomyopathies: 40 (3.4%) patients with left ventricular non-compaction, 17 (1.4%) with hypertrophic cardiomyopathy, and 10 (0.8%) with dilated cardiomyopathy. BAV subjects with hypertrophic cardiomyopathy had higher prevalences of diabetes mellitus and heart failure with preserved ejection fraction, and tended to have type 0 phenotype, while BAV subjects with dilated cardiomyopathy showed higher prevalences of chronic kidney disease and heart failure with reduced ejection fraction. BAV subjects with left ventricular non-compaction were significantly younger and predominantly male, and had greater BAV dysfunction and a higher prevalence of normal aorta shape. In multiple regression analysis, cardiomyopathy was independently associated with heart failure (odds ratio 2.795, 95% confidential interval 1.603-4.873, p<0.001) after controlling for confounding factors.
CONCLUSION
Concomitant cardiomyopathies were observed in 5.6% of subjects with BAV. A few different clinical and echocardiographic characteristics were found. The presence of cardiomyopathy was independently associated with heart failure.
MeSH Terms
Figure
-
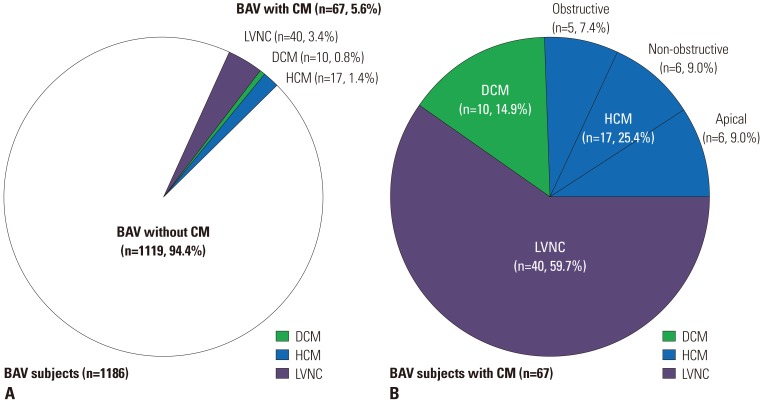
Fig. 1 Prevalence of specific cardiomyopathies in bicuspid aortic valves (BAV) subjects. (A) A total of 1186 BAV subjects. (B) Sixty-seven BAV subjects with cardiomyopathy (CM). LVNC, left ventricular non-compaction; DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy.
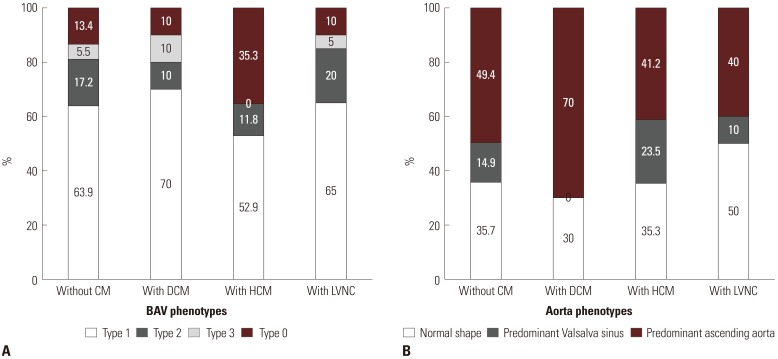
Fig. 2 (A) Bicuspid aortic valves (BAV) phenotypes according to the presence of specific cardiomyopathies (CMs). (B) Aorta phenotypes according to the presence of specific CMs. DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy; LVNC, left ventricular non-compaction.
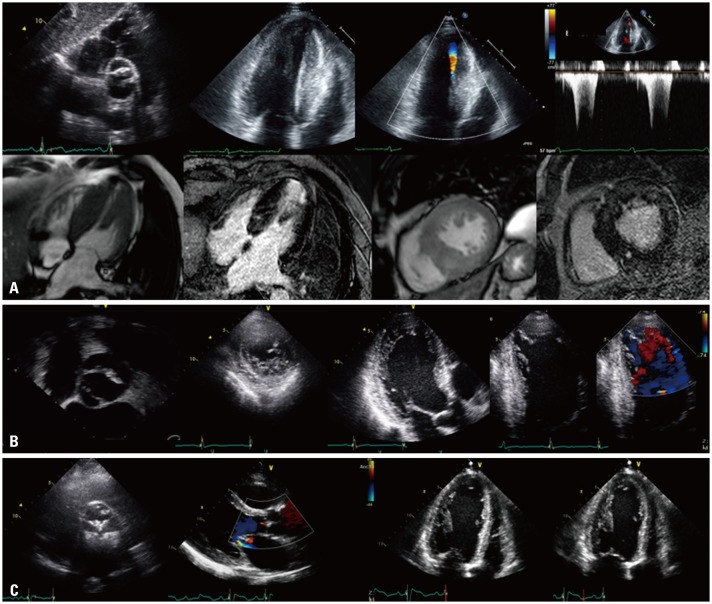
Fig. 3 Representative cases of coexisting cardiomyopathies in bicuspid aortic valves subjects. (A) Hypertrophic cardiomyopathy, (B) left ventricular non-compaction, and (C) dilated cardiomyopathy.
Reference
-
1. Ward C. Clinical significance of the bicuspid aortic valve. Heart. 2000; 83:81–85. PMID: 10618341.
Article2. Prakash SK, Bossé Y, Muehlschlegel JD, Michelena HI, Limongelli G, Della Corte A, et al. A roadmap to investigate the genetic basis of bicuspid aortic valve and its complications: insights from the international BAVCon (Bicuspid Aortic Valve Consortium). J Am Coll Cardiol. 2014; 64:832–839. PMID: 25145529.3. Shim CY, Cho IJ, Yang WI, Kang MK, Park S, Ha JW, et al. Central aortic stiffness and its association with ascending aorta dilation in subjects with a bicuspid aortic valve. J Am Soc Echocardiogr. 2011; 24:847–852. PMID: 21652174.
Article4. Kim M, Shim CY, You SC, Cho IJ, Hong GR, Ha JW, et al. Characteristics of carotid artery structure and mechanical function and their relationships with aortopathy in patients with bicuspid aortic valves. Front Physiol. 2017; 8:622. PMID: 28970802.
Article5. Niaz T, Poterucha JT, Johnson JN, Craviari C, Nienaber T, Palfreeman J, et al. Incidence, morphology, and progression of bicuspid aortic valve in pediatric and young adult subjects with coexisting congenital heart defects. Congenit Heart Dis. 2017; 12:261–269. PMID: 27893194.
Article6. Niaz T, Poterucha JT, Olson TM, Johnson JN, Craviari C, Nienaber T, et al. Characteristic morphologies of the bicuspid aortic valve in patients with genetic syndromes. J Am Soc Echocardiogr. 2018; 31:194–200. PMID: 29191731.
Article7. Lee SY, Shim CY, Hong GR, Seo J, Cho I, Cho IJ, et al. Association of aortic phenotypes and mechanical function with left ventricular diastolic function in subjects with normally functioning bicuspid aortic valves and comparison to subjects with tricuspid aortic valves. Am J Cardiol. 2015; 116:1547–1554. PMID: 26409638.8. Weismann CG, Lombardi KC, Grell BS, Northrup V, Sugeng L. Aortic stiffness and left ventricular diastolic function in children with well-functioning bicuspid aortic valves. Eur Heart J Cardiovasc Imaging. 2016; 17:225–230. PMID: 26072912.
Article9. Lee SY, Shim CY, Hong GR, Cho IJ, Chang HJ, Ha JW, et al. Determinants and prognostic significance of symptomatic status in patients with moderately dysfunctional bicuspid aortic valves. PLoS One. 2017; 12:e0169285. PMID: 28060855.
Article10. Feizi O, Farrer Brown G, Emanuel R. Familial study of hypertrophic cardiomyopathy and congenital aortic valve disease. Am J Cardiol. 1978; 41:956–964. PMID: 565586.
Article11. Brown PS Jr, Roberts CS, McIntosh CL, Roberts WC, Clark RE. Combined obstructive hypertrophic cardiomyopathy and stenotic congenitally bicuspid aortic valve. Am J Cardiol. 1990; 66:1273–1275. PMID: 2239738.
Article12. Agarwal A, Khandheria BK, Paterick TE, Treiber SC, Bush M, Tajik AJ. Left ventricular noncompaction in patients with bicuspid aortic valve. J Am Soc Echocardiogr. 2013; 26:1306–1313. PMID: 24044978.
Article13. Padang R, Gersh BJ, Ommen SR, Geske JB. Prevalence and impact of coexistent bicuspid aortic valve in hypertrophic cardiomyopathy. Heart Lung Circ. 2018; 27:33–40. PMID: 28377231.
Article14. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2015; 16:233–270. PMID: 25712077.
Article15. Lee SY, Shim CY, Kim D, Cho I, Hong GR, Ha JW, et al. Factors determining aortic valve dysfunction in Korean subjects with a bicuspid aortic valve. Am J Cardiol. 2017; 119:2049–2055. PMID: 28434646.
Article16. Roberts WC, Ko JM. Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation. Circulation. 2005; 111:920–925. PMID: 15710758.
Article17. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD, Levine RA, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003; 16:777–802. PMID: 12835667.
Article18. Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009; 22:1–23. PMID: 19130998.
Article19. Jenni R, Oechslin E, Schneider J, Attenhofer Jost C, Kaufmann PA. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart. 2001; 86:666–671. PMID: 11711464.
Article20. Chin TK, Perloff JK, Williams RG, Jue K, Mohrmann R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation. 1990; 82:507–513. PMID: 2372897.
Article21. Stöllberger C, Finsterer J, Blazek G. Left ventricular hypertrabeculation/noncompaction and association with additional cardiac abnormalities and neuromuscular disorders. Am J Cardiol. 2002; 90:899–902. PMID: 12372586.
Article22. Petersen SE, Timperley J, Neubauer S. Left ventricular thrombi in a patient with left ventricular non-compaction in visualisation of the rationale for anticoagulation. Heart. 2005; 91:e4. PMID: 15604311.
Article23. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Colvin MM, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA Guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017; 70:776–803. PMID: 28461007.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparable Outcomes of Bicuspid Aortic Valves for RapidDeployment Aortic Valve Replacement
- Coronary Alignment by the OctaAlign Technique Using a Myval Octacor Transcatheter Heart Valve in a Bicuspid Aortic Valve: A Case Report
- Three Cases of Ascending Aortic Aneurysm combined with Bicuspid Aortic Valve
- Transesophageal Echocardiographic Estmiation of Aortic Valve Area in Aortic Stenosis : A Comparison of Multiplane and Biplane Transesophageal Approach
- A Study of Pure Aortic Valvular Stenosis in Adult
