Transesophageal Echocardiographic Estmiation of Aortic Valve Area in Aortic Stenosis : A Comparison of Multiplane and Biplane Transesophageal Approach
- Affiliations
-
- 1Department of Internal Medicine, School of Medicine, Keimyung University, Taegu, Korea.
- 2Division of Cardiovascular Disease, University of Alabama at Birmingham, Alabama, USA.
- KMID: 2410445
- DOI: http://doi.org/10.4250/jkse.1994.2.2.170
Abstract
- BACKGROUND
There have been few reports in the literature evaluating aortic valve area by multiplane transesophageal echocardiography(M-TEE) as well as Biplane TEE(B-TEE) in comparison with transthoracic echocardiography(TTE) and cardiac catheterization(CC) estimated aortic valve area. The pupose of this study was to evaluate assessment of aortic valve area in patients with aortic stenosis by M-TEE compared to B-TEE and TTE. METHOD: 145 patients with known aortic valve stenosis underwent TTE, CC and intraoperative TEE assessment of the aortic valve area. 81 were done with multiplane only, 64 were done with biplane only. Results were compared with valve areas determined invasively by Gorlin formula and noninvasively by TTE using simplified continuity equation, TEE using direct planimetry and TEE proximal stenotic jet width. Aortic valve areas were also compared in sugically confirmed bicuspid and tricuspid aortic valves seperately.
RESULTS
The feasibility of TTE, M-TEE, B-TEE and JW were 95.2%, 100%, 87.5% and 95.9%, respectively. Correlation between valve areas determined by Gorlin equation and M-TEE was the highest(r=0.89, n=81). This was higher for bicuspid valves(r=0.93, n=32) than tricuspid aortic valves(r=0.87, n=48). Correlations between the area determined by the Gorlin equation and that determined by B-TEE(r=0.74, n=56) and TTE(r=0.66, n=138) were lower. Coreelation for bicuspid and tricuspid were also lower(r=0.77, n=23, and r=0.75, n=30, respectively in biplane assessment, and r=0.71, n=61, and r=0.65, n=73, respectively in TTE assessment). Correlation of invasively determined valve areas with JW was lowest(r=0.57, n=139) though bicuspid valve area correlated better(r=0.64, n=60)than tricuspid aortic valves(r=0.53, n=75).
CONCLUSION
M-TEE is superior to B-TEE in the assessment of aortic valve stenosis. Bicuspid aortic valve areas were accurately measured more consistently than tricuspid aortic valve areas. M-TEE can be used addiotional method to evaluate aortic valve area with conventional TEE and cardiac catheterization.
MeSH Terms
Figure
-

Fig. 1. Aortic valve area measured by direct planimetric method using multiplane transesophageal echocardiography The scanning plane was 38 degree and valve area was 0.9cm2.
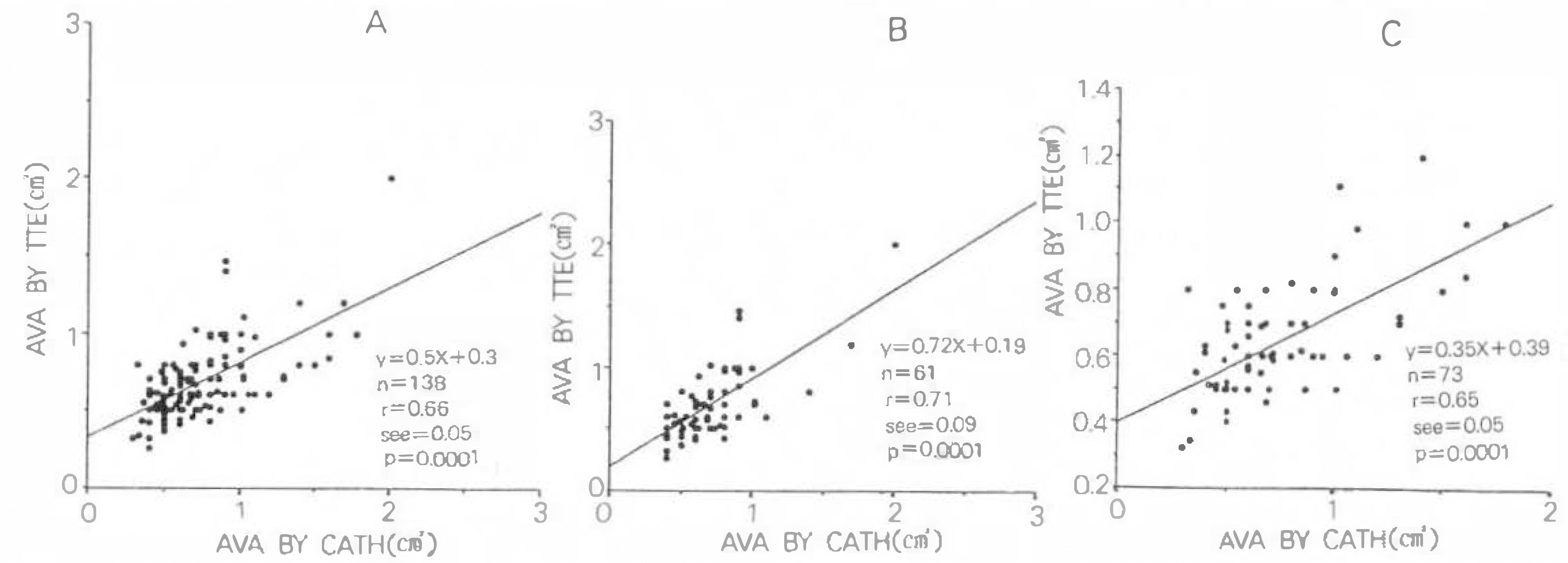
Fig. 2. Linear regression analysis of aortic valve areas (AVA) determined by simplified continuity equation and determined by Gorlin equation. A: Comparision of AVA in total patients. B: Comparision of AVA in bicuspid aortic valve stenosis. C: Comparision of AVA in tricuspid aortic valve stenosis.
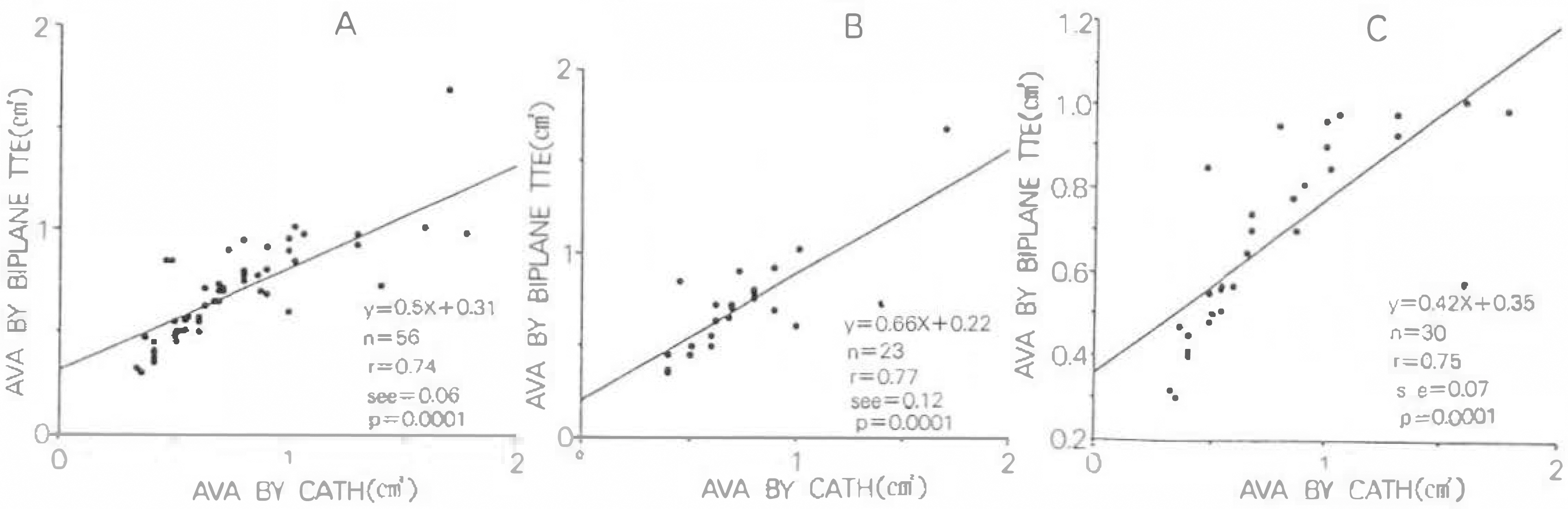
Fig. 3. Linear regression analysis of aortic valve areas determined by biplane transesophageal echocardiography and determined by Gorlin equation. A: Comparision of AVA in total patients. B: Comparision of AVA in bicuspid aortic valve stenosis. C: Comparision of AVA in tricuspid aortic valve stenosis.

Fig. 4. Linear regression analysis of aortic valve areas determined by multiplane transesophageal echocardiography and determined by Gorlin equation. A: Comparision of AVA in total patients. B: Comparision of AVA in bicuspid aortic valve stenosis. C: Comparision of AVA in tricuspid aortic valve stenosis.

Fig. 5. Linear regression analysis of aortic valve areas determined by stenotic jet width and determined by Gorlin equation. A: Comparision of AVA in total patients. B: Comparision of AVA in bicuspid aortic valve stenosis. C: Comparision of AVA in tricuspid aortic valve stenosis.
Reference
-
References
1). Godley RW, Green D, Dillon JC, Rogers EW, Feigenbaum H. Reliability of two-dimensional echocardiography in assessing the severity of valvular aortic stenosis. Chest. 79:657. 1981.
Article2). DeMaria AN, Bommer W, Joye J, Lee G, Bouteller J, Mason DT. Value and limitation of cross-sectional echocardiography of the aortic valve in the diagnosis and quantification of valvular aortic stenosis. Circulation. 62:304. 1980.3). Teirstein P, Yearger M, Yock PG. Doppler echocardiographic measurement of aortic valve area in aortic stenosis: A noninvasive application of the Gorlin formula. J Am Coll Cardiol. 8:1059. 1986.
Article4). Stamm RB, Martin R. Quantification of pressure gradients accross stenotic valves by Doppler ultrasound. J Am Coll Cardiol. 2:707. 1983.5). Galan A, Zoghbi WA, Quinones MA. Determination of severity of valvular aortic stenosis by Doppler echocardiography and relation of findings to clinical outcome and assessment with hemodynamic measurements determined at cardiac catheterization. Am J Cardiol. 67:1007. 1991.6). Currie PJ, Seward JB, Reeder GS, Vlietstra RE, Bresnahan DR, Bresnahan JF, Smith HC, Hagler DJ, Tajik AJ. Continous-wave Doppler echocardiographic assessment of severity of calcific aortic stenosis: a simultaneous Doppler-catheterization correlative study in 100 adult patients. Circulation. 71:1162. 1985.7). Smith MD, Dawson PL, Elion JL, Booth DC, Handshoe R, Kwan OL, Earle GF, DeMaria AN. Correlation of continuity wave Doppler velocity with cardiac catheterization gradients: an experimental model of aortic stenosis: J Am Coll Cardiol. 6:1306. 1985.8). Danielsen R, Nordrehaug JE, Stangel L, Vik-Mo H. Limitation in assessing the severity of aortic stenosis by Doppler gradients. Br Heart J. 59:551. 1988.9). Skiaerpe T, Hegrenase L, Hatle L. Noninvasive estimation of valve area in patients with aortic stenosis by Doppler ultrasound and two-dimensional echocardiography. Circulation. 72:810. 1985.
Article10). Zoghbi WA, Farmer KL, Soto JG, Nelson JG, Quinones MA. Accurate noninvasive quantification of stenotic aortic valve area by Doppler echocardiography. Circulation. 73:452. 1986.
Article11). Richards KL, Cannon SR, Miller jf, Crawford MH. Calculation of aortic valve area by Doppler echocardiography: a direct application of the continuity equation. Circulation. 73:964. 1986.
Article12). Oh JK, Taliercio CP, Holmes DR, Reeder GS, Bailey KB, Seward JB, Tajik AJ. Prediction of the severity of aortic stenosis by Doppler aortic valve area determination: Prospective Doppler-catheterization correlation in 100 patients. J Am Coll Cardiol. 11:1227. 1988.
Article13). Hofman T, Kasper W, Meinertz T, Spillner G, Schlosser V, Just H. Determination of aortic valve area in aortic stenosis by two-dimensional transesophageal echocardiography. Am J Cardiol. 59:330. 1987.14). Stoddard MF, Arce J, Liddel NE, Peters G, Dillon S, Kupersmith J. Two-dimensional transesophageal echocardiographic determination of aortic valve area in adults with aortic stenosis. Am Heart J. 122:1415. 1991.
Article15). Chandrsekaran K, Foley R, Weintraub A. Evidence that transesophageal echocardiography can reliably and directly measure the aortic valve area in patients with aortic stenosis-a new application that is independant of LV function and dose not require Doppler data(abst). J Am Coll Cardiol. 17(supp A):20A. 1991.16). Hoffman R, Flachskampf F, Hanrath P. Planimetry of orifice area in aortic stnosis using multiplane transesophageal echocardiography. J Am Coll Cardiol 22y. 529–1993.17). Tribouilloy C, Shen WF, Peltier M, Mirode A, Rey JL, Lesbre JP. Quantification of aortic valve area in aortic stenosis with multiplane transesophageal echocardiography: Comparsion with monoplane transesophageal approach. Am Heart J. 128:525. 1994.18). Perry GJ, Helmcke F, Nanda NC, Byard C, Soto B. Evaluation of aortic insuffiency by Doppler color flow mapping. J Am Coll Cardiol. 9:952. 1987.19). Fan P, Kapur K, Nanda NC. Color-guided echocardiographic assessment of aortic valve stenosis. J Am Coll Cardiol. 12:441. 1988.20). Baumgartner H, Kratzer H, Helmreiche G, Kuehn P. Determination of aortic valve area by Doppler echocardiography using the continuity equation: A critical evaluation. Cardiology. 71:101. 1990.
Article21). Judge KW, Otto CM. Doppler echocardiographic evaluation of aortic stenosis. Cardiol Clinics. 8:203. 1990.22). Otto CM, Pearlman AS. Doppler echocardiography in adults with symptomatic aortic stenosis. Arch Intern Med. 148:2553. 1988.
Article23). Burwash IG, Thomas DD, Sadahiro M, Pearlman AS, Verrier ED, Thomas R, Kraft CD, Otto CM. Dependence of Gorlin Formula and contnity equation valve area on transvalvular volume flow rate in valvular aortic stenosis. Circulation. 89:827. 1994.24). Lange H, Hasbrouck K, Olson J, et al. Comparison of transesophageal and transthoracic echocardiography for the assessment of the elderly. International symposium: Cardiovascular ultrasound application of new technique. Mayo Clinic;September 1989.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiplane Transesophageal Echocardiographic Findings of Two Cases of Discrete Subvalvular Aortic Stenosis
- Left Atrial Dissection by Aorto-Left Atrial Fistula after Aortic Valve Replacement: A case report
- A Case of 51 Year Old Woman with Quadricuspid Aortic Valve Associated with Regurgitation
- Bentall Operation in a Patient with a Unicommissural Unicuspid Aortic Valve
- Echocardiography in Transcatheter Aortic Valve Implantation and Mitral Valve Clip
