A Case of Subcutaneous and Intranasal Phaeohyphomycosis Caused by Microsphaeropsis arundinis in an Immunocompromised Patient Misdiagnosed with Mucormycosis
- Affiliations
-
- 1Department of Dermatology, School of Medicine, Chosun University, Gwangju, Korea. chna@chosun.ac.kr
- KMID: 2456237
- DOI: http://doi.org/10.5021/ad.2019.31.5.571
Abstract
- Microsphaeropsis arundinis is a dematiaceous fungus capable of causing soft tissue infections known as phaeohyphomycosis, mostly in immunocompromised individuals. These infections arise from the traumatic inoculation of fungal materials into the subcutis, and can spread to adjacent subcutaneous tissues or via the lymphatics in a sporotrichoid manner. A 76-year-old man presented with diffuse erythematous plaques and swelling on both forearms and dorsal hands, and rhinalgia. He had been undergoing treatment for hypertension, angina pectoris, and diabetes. Histopathologic examinations of the skin, painful nasal septum, and molecular identification using internal transcribed spacer regions confirmed a diagnosis of subcutaneous and intranasal phaeohyphomycosis caused by M. arundinis. The patient was treated with oral itraconazole for over 5 months, and no recurrence was observed until the time of writing this manuscript. We report a rare case of subcutaneous and intranasal phaeohyphomycosis caused by M. arundinis and propose that confirmation of the causative strains is necessary, as it could affect the prognosis and treatment of the disease.
MeSH Terms
Figure
-
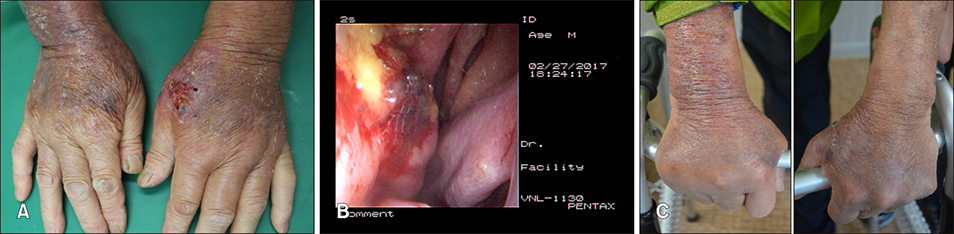
Fig. 1 (A) Diffuse purulent erythematous plaques and swelling with scales and pustules on both dorsal hands and forearms of the patient; (B) necrotic changes in the nasal septum with hemorrhage and exudate; (C) and completely recovered lesions after treatment with itraconazole for 5 months.
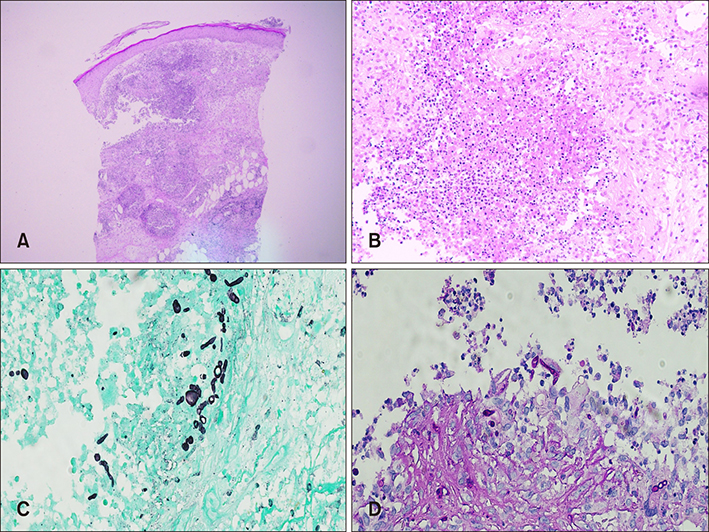
Fig. 2 (A, B) Dense infiltrates of inflammatory cells such as neutrophils, monocytes, histiocytes, and giant cells extending from the upper dermis through the subcutaneous fatty layer (H&E: A, ×40; B, ×200); (C, D) Gomori's methenamine silver (GMS) staining and periodic acid-Schiff (PAS) staining revealed fungal hyphae and spores (C: GMS, ×400, D: PAS, ×400).
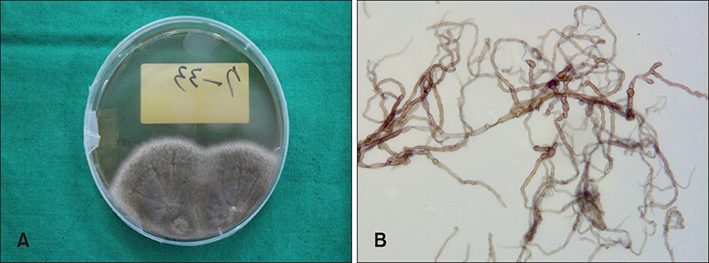
Fig. 3 (A) Microsphaeropsis arundinis colonies growing on Sabouraud dextrose agar at 30℃ demonstrating gray to dark green colonies (14 days); (B) microscopic morphology of M. arundinis stained with lactophenol cotton blue showing pigmented, septate, and irregularly formed hyphae, with swollen segments.
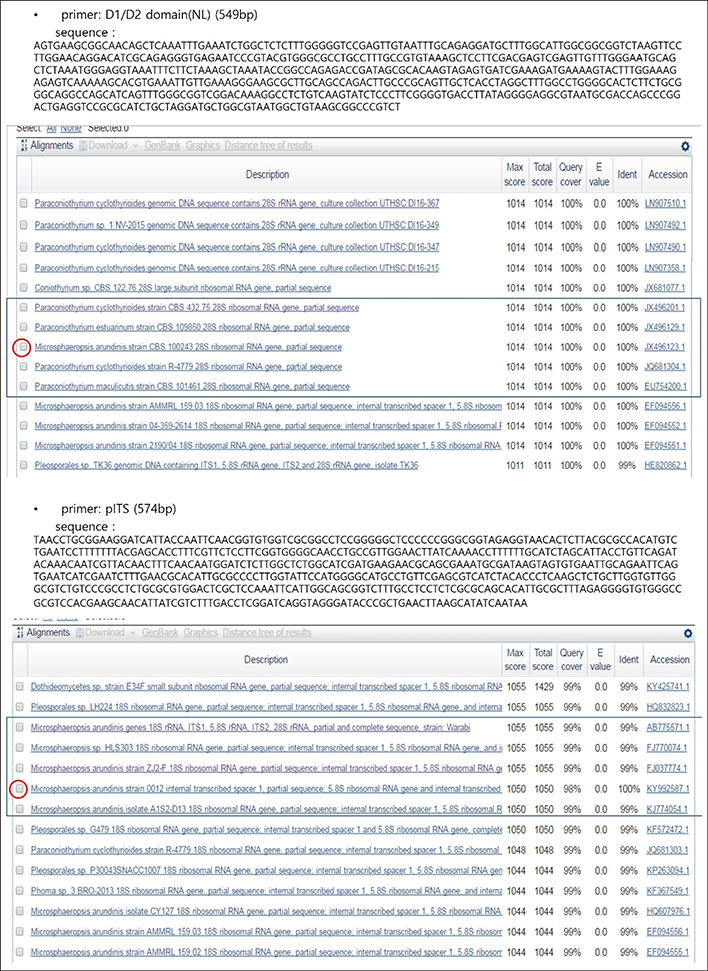
Fig. 4 The sequence of the D1/D2 domain of ribosomal RNA gene regions and ITS1-5.8S-ITS2 regions showed identity with Microsphaeropsis arundinis (100% sequence identity to M. arundinis CBS 100243 [GenBank accession number JX 496123.1] and 100% sequence identity to M. arundinis 0012 [GenBank accession number KY992587.1]).
Reference
-
1. Pendle S, Weeks K, Priest M, Gill A, Hudson B, Kotsiou G, et al. Phaeohyphomycotic soft tissue infections caused by the coelomycetous fungus Microsphaeropsis arundinis. J Clin Microbiol. 2004; 42:5315–5319.
Article2. Asahina A, Kobayashi M, Nakano K, Saito I, Yarita K, Kamei K, et al. Deep cutaneous infection with Microsphaeropsis arundinis: report of two Japanese cases. Acta Derm Venereol. 2015; 95:855–857.
Article3. Hall MR, Brumble LM, Mayes MA, Snow JL, Keeling JH. Cutaneous Microsphaeropsis arundinis infection initially interpreted as squamous cell carcinoma. Int J Dermatol. 2013; 52:84–86.
Article4. Kim MN, Shin JH, Sung H, Lee K, Kim EC, Ryoo N, et al. Candida haemulonii and closely related species at 5 university hospitals in Korea: identification, antifungal susceptibility, and clinical features. Clin Infect Dis. 2009; 48:e57–e61.5. Crawford SJ, Chen SC, Halliday C, Rangan GK, Gottlieb T, Reid AB. Microsphaeropsis arundinis skin and soft tissue infection in renal transplant recipients: three case reports and a review of the literature. Transpl Infect Dis. 2015; 17:915–920.
Article6. Lee KC, Kim MJ, Chae SY, Lee HS, Jang YH, Lee SJ, et al. A case of phaeohyphomycosis caused by Exophiala lecaniicorni. Ann Dermatol. 2016; 28:385–387.
Article7. Ryu TH, Kwon IH, Choi JE, Ahn HH, Kye YC, Seo SH. A case of subcutaneous phaeohyphomycosis caused by Exophiala oligosperma showing multiple cysts. Korean J Dermatol. 2017; 55:259–263.8. Suh MK, Kwon SW, Kim TH, Sun YW, Lim JW, Ha GY, et al. A case of subcutaneous phaeohyphomycosis caused by Exophiala jeanselmei. Korean J Dermatol. 2005; 43:124–127.9. Ajello L, Georg LK, Steigbigel RT, Wang CJ. A case of phaeohyphomycosis caused by a new species of Phialophora. Mycologia. 1974; 66:490–498.
Article10. Sutton DA. Coelomycetous fungi in human disease. A review: clinical entities, pathogenesis, identification and therapy. Rev Iberoam Micol. 1999; 16:171–179.11. Stchigel AM, Sutton DA. Coelomycete fungi in the clinical lab. Curr Fungal Infect Rep. 2013; 7:171–191.
Article12. Chowdhary A, Meis JF, Guarro J, de Hoog GS, Kathuria S, Arendrup MC, et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of systemic phaeohyphomycosis: diseases caused by black fungi. Clin Microbiol Infect. 2014; 20 Suppl 3:47–75.
Article13. Ostrosky-Zeichner L, Alexander BD, Kett DH, Vazquez J, Pappas PG, Saeki F, et al. Multicenter clinical evaluation of the (1--〉3) beta-D-glucan assay as an aid to diagnosis of fungal infections in humans. Clin Infect Dis. 2005; 41:654–659.
Article14. Perusquía-Ortiz AM, Vázquez-González D, Bonifaz A. Opportunistic filamentous mycoses: aspergillosis, mucormycosis, phaeohyphomycosis and hyalohyphomycosis. J Dtsch Dermatol Ges. 2012; 10:611–621. quiz 621-622.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Subcutaneous Phaeohyphomycosis Caused by Exophiala oligosperma Showing Multiple Cysts
- Phaeohyphomycosis Due to Exophiala dermatitidis Successfully Treated with Itraconazole
- A Case of Rhinocerebral Mucormycosis Misdiagnosed as Herpes Zoster
- The First Case of Phaeohyphomycosis Caused by Exophiala xenobiotica in an Immunocompetent Patient in Korea
- A Case of Nasal Septal and Oral Cavity Abscesses Resulting from Mucormycosis in an Immunocompromised Patient
