Effects of insulin and metformin on fetal kidney development of streptozotocin-induced gestational diabetic albino rats
- Affiliations
-
- 1Department of Anatomy, Faculty of Medicine, Suez Canal University, Ismailia, Egypt. omima34@hotmail.com
- KMID: 2451220
- DOI: http://doi.org/10.5115/acb.2019.52.2.161
Abstract
- Gestational diabetes mellitus is one of common medical complications of pregnancy. Hyperglycemia in utero impairs renal development and produces renal anomalies. Metformin has antioxidant properties and better glycemic control. Aim: assessment insulin and metformin effects on renal development of streptozotocin-induced gestational diabetic albino rats. Sixty virgin female albino rats were used. Once pregnancy confirmed, animals were randomly assigned into control, metformin, diabetic, diabetic plus insulin, diabetic plus metformin and diabetic plus insulin and metformin treated groups. Rats were sacrificed on the 20th day of gestation; fetuses were extracted and weighted. Fetal kidneys were extracted prepared for light, morphometric and electron microscopic examination. Diabetic followed by diabetic plus metformin treated groups revealed retardation of glomerular development in the cortical and Juxtaglomerular zones with a significant increase in the early immature glomerular stages and immature to mature glomerular ratio compared to other groups. Diabetic group also showed morphometric changes, shrunken and empty glomeruli, vacuolar degeneration and hemorrhage. Diabetic plus metformin group showed minimal improvement while diabetic plus insulin and diabetic plus insulin and metformin groups showed developmental, histopathological and morphometric improvement with best results in the combination group. Gestational diabetes mellitus (GDM) possess deleterious effects on fetal kidney development. Insulin improves the glycemic state and decreases GDM effects on fetal kidneys. Metformin produces mild protection while the combination of insulin and metformin produces the best glycemic control and protect fetal kidneys.
MeSH Terms
Figure
-

Fig. 1 Values of maternal random blood sugar throughout gestation in the studied groups. +ve, positive control; −ve, negative control.
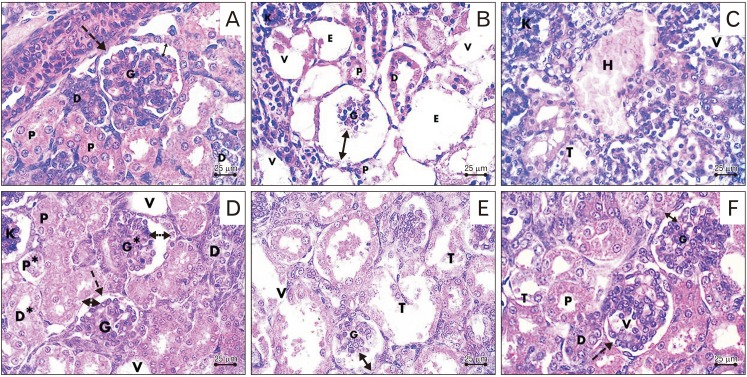
Fig. 2 Photomicrographs sections in the fetal kidney. (A) Control group showing the renal corpuscle with the parietal layer of Bowman's capsule (dashed arrow), mature glomerulus (G) and preserved corpuscular space (double head arrow), proximal (P) and distal (D) convoluted tubules. (B, C) Diabetic group showing shrunken glomerulus (G), increased renal corpuscular space (double head arrow), vacuolations (V), empty renal corpuscles (E), degenerated dilated tubules (T), shedding of brush border of proximal tubules (P), degenerated epithelium of distal tubule (D), hemorrhage (H) and pyknotic nuclei (K). (D) Diabetic plus insulin-treated group showing intact mature glomeruli (G) surrounded by Bowman's capsule (dashed arrow) with preserved corpuscular space (double head arrow), intact proximal (P) and distal tubules (D). Notice the presence of mildly shrunken glomerulus (G*), pyknotic nuclei (K), increased corpuscular space (double head dashed arrow), degenerated proximal (P*) and distal convoluted tubules (D*) and areas of vacuolation (V). (E) Diabetic plus metformin-treated group showing shrunken mature glomerulus (G), increased renal corpuscular space (double head arrow), dilated and destructed renal tubules (T), and vacuolation (V). (F) Diabetic plus insulin and metformin-treated group showing intact glomeruli (G), Bowman's capsule (dashed arrow), and preserved corpuscular space (double head arrow), intact proximal (P) and distal (D) convoluted tubules. Notice the presence of areas of vacuolation in the glomerulus (V) and tubules (T) (H&E staining, ×400).

Fig. 3 Periodic acid-Schiff stained sections in the fetal kidney. (A) Control group showing positive stain in the glomeruli (G), Bowman's capsule (arrowhead), basement membrane of renal tubules (arrow) and the brush border of proximal tubules (dashed arrow). (B) Diabetic group showing faint reaction in glomeruli (G), Bowman's capsules (arrowheads), basement membrane (dashed arrows) and brush border of the proximal convoluted tubules (arrows). (C) Diabetic plus insulin treated group showing positive reaction in the glomeruli (G), Bowman's capsule (arrowheads), basement membrane of renal tubules (arrow) and the brush border of proximal tubules (dashed arrow). Notice the presence of areas of negative reaction (stars). (D) Diabetic plus metformin treated group showing areas of faint reaction in the tubular basement membrane (arrow) and glomerulus (dashed arrow) with the presence of positive reaction in other glomerulus (G) and Bowman's capsule (arrowhead). (E) Diabetic plus insulin and metformin treated group showing positive reaction in the glomerulus (G), Bowman's capsule (arrowhead), basement membrane of renal tubules (arrows) and the brush border of proximal tubules (dashed arrows) (periodic acid-Schiff, ×400).

Fig. 4 Photomicrographs of Toluidine blue stained sections in the fetal kidney. (A–C) Control group showing vesicle (V), S-shaped (S), commashaped (Co), and capillary loop (CL) stages of glomerular development. (D) Control group showing mature glomerulus (G) with the parietal layer of Bowman's capsule (BC), podocyte (Pd), mesangial cells (M), proximal convoluted tubules (P) and distal (D) convoluted tubules. (E) Diabetic group showing, loss in the normal architecture of the cortex, immature glomerulus (vesicular stage) (G) and marked vacuolations (V) within the glomerulus and tubules. (F) Diabetic plus insulin-treated group showing intact mature glomerulus (G), proximal (P) and distal (D) convoluted tubules. Notice small area of hemorrhage (H) and vacuolation (arrow). (G) Diabetic plus metformin-treated group showing shrunken glomerulus (G), wide Bowman's space (BS), and areas of hemorrhage (H). Notice degenerated tubules (T). (H) Diabetic plus insulin and metformin-treated group showing intact mature renal glomerulus (G), Bowman's capsule (BC), podocyte (Pd), proximal (P) and distal (D) convoluted tubules (toluidine blue, ×1,000).
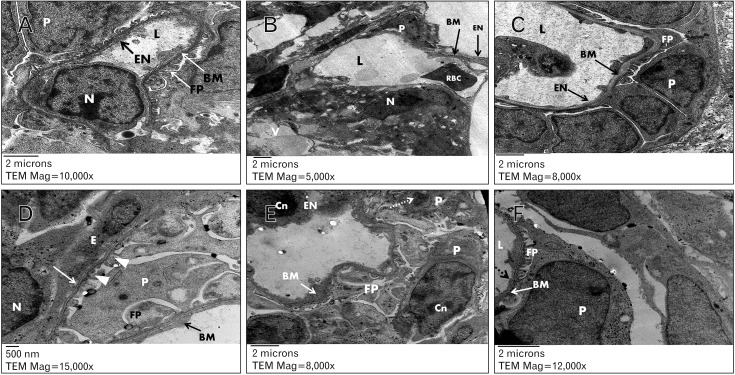
Fig. 5 Electron photomicrographs in fetal rat glomerulus. (A) Control group showing glomerular capillary lumen (L) lined with endothelial cell with euchromatic nucleus (N) and forming a thin fenestrated layer of cytoplasm (EN) lining the basement membrane (BM) internally. The capillary surrounded with intact podocyte (P) with foot processes (FP). Uranyl acetate and lead citrate (×10,000). (B) Diabetic group showing glomerular capillary lumen (L) with thinned glomerular filtration barrier (BM) and red blood cell (RBC), absence of fenestrations of endothelial layer (EN), vacuolations (V), podocytes with loss of foot processes (P) and chromatin clumping (N). Uranyl acetate and lead citrate, ×5,000. (C) Diabetic group showing glomerular capillary lumen (L) with a thickened glomerular basement membrane (BM) and area of absence of EN and surrounded by podocyte (P) with short foot process effacement and widening (FP). Uranyl acetated and lead citrate, ×8,000. (D) Diabetic plus insulin-treated group showing capillary endothelial cell (E) with euchromatic nucleus (N), podocyte (P) with intact foot processes (arrowheads) and homogeneous glomerular basement membrane with normal thickness (white arrow). Other areas of thickened glomerular basement membrane (BM) and marked widening and effacement of foot processes (FP). Uranyl acetate and lead citrate, ×15,000. (E) Diabetic plus metformin-treated group showing area of thick glomerular basement membrane (BM) and chromatin condensation (Cn) in nuclei of capillary endothelial cell (EN) and podocytes (P). Notice the presence of ill-defined nuclear envelop (dashed arrow) and foot process with effacement and widening (FP). Uranyl acetate and lead citrate, ×8,000. (F) diabetic plus insulin and metformin-treated group showing glomerular capillary lumen (L), intact glomerular basement membrane (BM), podocytes (P) with narrow and short foot processes (FP), thin layer of cytoplasmic endothelium with characteristic interruptions (dashed arrow). Uranyl acetate and lead citrate, ×12,000.
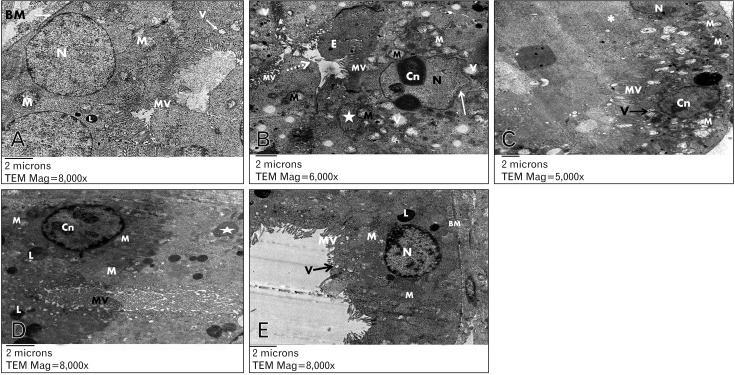
Fig. 6 Electron photomicrographs in the proximal convoluted tubule epithelial cells of fetal rat kidney. (A) Control group showing basal euochromatic nucleus (N), apical brush border with closely packed microvilli (MV), pinocytic vesicles (V), lysosome (L), plenty of mitochondria (M) and basement membrane (BM). Uranyl acetate and lead citrate, ×8,000. (B) Diabetic group showing irregular shaped nucleus (N), ill-defined and irregular nuclear envelope (white arrow), chromatin condensation (Cn), apical sticky and profoundly thin microvilli (MV) with areas of total loss of brush border (dashed arrow), swollen mitochondria with disruption of cristae (M) and apoptotic body (star). Notice presence of pinocytotic vesicles (V), and the lumen filled with exudate (E). Uranyl acetate and lead citrate, ×6,000. (C) Diabetic plus insulin treated group showing closely packed apical long microvilli (MV), euochromatic nucleus (N) and plenty of mitochondria (M). Notice the presence of areas with microvilli loss (*), vesicles (V), and nucleus with chromatin condensation (Cn). Uranyl acetate and lead citrate, ×5,000. (D) Diabetic plus metformin treated group showing plenty of lysosomes (L), edematous mitochondria (M), nucleus with chromatin condensation (Cn), apoptotic body (star) and apical profoundly thin and sloughed microvilli (MV). Uranyl acetate and lead citrate, ×8,000. (E) Diabetic plus insulin and metformin-treated group showing closely packed apical microvilli (MV), pinocytic vesicles (V), lysosomes (L), euchromatic nucleus (N), plenty of mitochondria (M) and intact basement membrane (BM). Uranyl acetate and lead citrate, ×8,000.

Fig. 7 Electron photomicrographs in the distal convoluted tubule epithelial cells of fetal rat kidney. (A) Control group showing with blunt microvilli (MV), rounded euchromatic nucleus (N) and plenty of mitochondria (M). Uranyl acetate and lead citrate, ×15,000. (B) Diabetic group showing lumen obliteration with exudate (E), few microvilli (MV), swollen and disrupted mitochondria (M), pinocytotic vesicles (V), apoptotic body (star) and nuclei with chromatin condensation (Cn). Uranyl acetate and lead citrate, ×8,000. (C) Diabetic plus insulin-treated group showing short apical microvilli (MV), euchromatic nucleus (N) while other nucleus showed chromatin condensation (Cn), swollen and disrupted mitochondria (M). Uranyl acetate and lead citrate, ×8,000. (D) Diabetic plus metformin-treated group showing ill-defined cell boundaries, swollen mitochondria (M) and destructed and ruptured nucleus (N). Uranyl acetate and lead citrate, ×8,000. (E) Diabetic plus insulin and metformin-treated group showing small microvilli (MV), euchromatic rounded nucleus (N) with chromatin condensation (Cn) and intact mitochondria (M). Uranyl acetate and lead citrate, ×8,000.
Reference
-
1. World Health Organization. Definition, diagnosis and classification of diabetes mellitus and its complications: report of a WHO consultation. Part 1. Diagnosis and classification of diabetes mellitus. Geneva: World Health Organization;1999.2. Scherzer P, Katalan S, Got G, Pizov G, Londono I, Gal-Moscovici A, Popovtzer MM, Ziv E, Bendayan M. Psammomys obesus, a particularly important animal model for the study of the human diabetic nephropathy. Anat Cell Biol. 2011; 44:176–185. PMID: 22025969.3. King AJ. The use of animal models in diabetes research. Br J Pharmacol. 2012; 166:877–894. PMID: 22352879.4. Winocour PH. Diabetes and chronic kidney disease: an increasingly common multi-morbid disease in need of a paradigm shift in care. Diabet Med. 2018; 35:300–305. PMID: 29247554.5. Buchanan TA, Xiang AH, Page KA. Gestational diabetes mellitus: risks and management during and after pregnancy. Nat Rev Endocrinol. 2012; 8:639–649. PMID: 22751341.6. Guariguata L, Linnenkamp U, Makaroff LE, Ogurtsova K, Colagiuri S. Global estimates of hyperglycaemia in pregnancy: determinants and trends. In : Rajendram R, Preedy VR, Patel VB, editors. Nutrition and Diet in Maternal Diabetes: An Evidence-Based Approach. Cham: Springer International Publishing;2018. p. 3–15.7. Fetita LS, Sobngwi E, Serradas P, Calvo F, Gautier JF. Consequences of fetal exposure to maternal diabetes in offspring. J Clin Endocrinol Metab. 2006; 91:3718–3724. PMID: 16849402.8. Graham DL, Schaefer TL, Vorhees CV. Neurobehavioral testing for developmental toxicity. In : Hood RD, editor. Developmental and Reproductive Toxicology: A Practical Approach. Boca Raton, FL: CRC Press;2016. p. 346–387.9. Alfadhli EM. Gestational diabetes mellitus. Saudi Med J. 2015; 36:399–406. PMID: 25828275.10. Pilmore HL. Review: metformin: potential benefits and use in chronic kidney disease. Nephrology (Carlton). 2010; 15:412–418. PMID: 20609092.11. Legro RS. Metformin during pregnancy in polycystic ovary syndrome: another vitamin bites the dust. J Clin Endocrinol Metab. 2010; 95:5199–5202. PMID: 21131540.12. Balani J, Hyer SL, Rodin DA, Shehata H. Pregnancy outcomes in women with gestational diabetes treated with metformin or insulin: a case-control study. Diabet Med. 2009; 26:798–802. PMID: 19709150.13. Rowan JA, Rush EC, Obolonkin V, Battin M, Wouldes T, Hague WM. Metformin in gestational diabetes: the offspring follow-up (MiG TOFU): body composition at 2 years of age. Diabetes Care. 2011; 34:2279–2284. PMID: 21949222.14. Othman EM, Oli RG, Arias-Loza PA, Kreissl MC, Stopper H. Metformin protects kidney cells from insulin-mediated genotoxicity in vitro and in male Zucker diabetic fatty rats. Endocrinology. 2016; 157:548–559. PMID: 26636185.15. Varayoud J, Ramos JG, Bosquiazzo VL, Lower M, Muñoz-de-Toro M, Luque EH. Neonatal exposure to bisphenol A alters rat uterine implantation-associated gene expression and reduces the number of implantation sites. Endocrinology. 2011; 152:1101–1111. PMID: 21285323.16. Amorim EM, Damasceno DC, Perobelli JE, Spadotto R, Fernandez CD, Volpato GT, Kempinas WD. Short- and long-term reproductive effects of prenatal and lactational growth restriction caused by maternal diabetes in male rats. Reprod Biol Endocrinol. 2011; 9:154. PMID: 22142502.17. Ikeda T, Iwata K, Murakami H. Inhibitory effect of metformin on intestinal glucose absorption in the perfused rat intestine. Biochem Pharmacol. 2000; 59:887–890. PMID: 10718348.18. Pan Y, Li YJ, Zhao HY, Zheng JM, Xu H, Wei G, Hao JS, Cui FD. Bioadhesive polysaccharide in protein delivery system: chitosan nanoparticles improve the intestinal absorption of insulin in vivo. Int J Pharm. 2002; 249:139–147. PMID: 12433442.19. Ellis EN, Steffes MW, Goetz FC, Sutherland DE, Mauer SM. Relationship of renal size to nephropathy in type 1 (insulin-dependent) diabetes. Diabetologia. 1985; 28:12–15. PMID: 3979681.20. Suvarna SK, Layton C, Bancroft JD. Bancroft's theory and practice of histological techniques. Philadelphia, PA: Elsevier Health Sciences;2012.21. Furuse A, Bernstein J, Welling LW, Welling DJ. Renal tubular differentiation in mouse and mouse metanephric culture. II. Na-K-ATPase activity. Pediatr Nephrol. 1989; 3:273–279. PMID: 2562015.22. Guariguata L, Linnenkamp U, Makaroff LE, Ogurtsova K, Colagiuri S. Global estimates of hyperglycaemia in pregnancy: determinants and trends. In : Rajendram R, Preedy VR, Patel VB, editors. Nutrition and Diet in Maternal Diabetes: Nutrition and Health. Cham: Humana Press;2018. p. 3–15.23. Shaw RJ, Lamia KA, Vasquez D, Koo SH, Bardeesy N, Depinho RA, Montminy M, Cantley LC. The kinase LKB1 mediates glucose homeostasis in liver and therapeutic effects of metformin. Science. 2005; 310:1642–1646. PMID: 16308421.24. Turner RC, Cull CA, Frighi V, Holman RR. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). UK Prospective Diabetes Study (UKPDS) Group. JAMA. 1999; 281:2005–2012. PMID: 10359389.25. Lund SS, Tarnow L, Frandsen M, Nielsen BB, Hansen BV, Pedersen O, Parving HH, Vaag AA. Combining insulin with metformin or an insulin secretagogue in non-obese patients with type 2 diabetes: 12 month, randomised, double blind trial. BMJ. 2009; 339:b4324. PMID: 19900993.26. Martinez CA. The ultrasound evaluation of the diabetic pregnancy. In : Moore L, editor. Diabetes in Pregnancy. Cham: Springer;2018. p. 163–181.27. Singh N, Madhu M, Vanamail P, Malik N, Kumar S. Efficacy of metformin in improving glycaemic control & perinatal outcome in gestational diabetes mellitus: a non-randomized study. Indian J Med Res. 2017; 145:623–628. PMID: 28948952.28. Taricco E, Radaelli T, Nobile de Santis MS, Cetin I. Foetal and placental weights in relation to maternal characteristics in gestational diabetes. Placenta. 2003; 24:343–347. PMID: 12657507.29. Ornoy A. Embryonic oxidative stress as a mechanism of teratogenesis with special emphasis on diabetic embryopathy. Reprod Toxicol. 2007; 24:31–41. PMID: 17548185.30. Liu F, Zhao C, Liu L, Ding H, Huo R, Shi Z. Peptidome profiling of umbilical cord plasma associated with gestational diabetes-induced fetal macrosomia. J Proteomics. 2016; 139:38–44. PMID: 26945739.31. Ainuddin JA, Karim N, Zaheer S, Ali SS, Hasan AA. Metformin treatment in type 2 diabetes in pregnancy: an active controlled, parallel-group, randomized, open label study in patients with type 2 diabetes in pregnancy. J Diabetes Res. 2015; 2015:325851. PMID: 25874236.32. Neves HM, Sgarbosa F, Calderon IM, Vianna LS, Santini AC, Sieiro Netto L, Dias A. Does hyperglycemia in pregnancy change fetal kidney growth? A longitudinal prospective study. Rev Bras Ginecol Obstet. 2013; 35:442–446. PMID: 24337055.33. Page NM, Kemp CF, Butlin DJ, Lowry PJ. Placental peptides as markers of gestational disease. Reproduction. 2002; 123:487–495. PMID: 11914111.34. Venkatachalam MA, Griffin KA, Lan R, Geng H, Saikumar P, Bidani AK. Acute kidney injury: a springboard for progression in chronic kidney disease. Am J Physiol Renal Physiol. 2010; 298:F1078–F1094. PMID: 20200097.35. Dodd SM. Tubulointerstitial and cystic disease of the kidney. Berlin: Springer Science & Business Media;2012.36. Kolset SO, Reinholt FP, Jenssen T. Diabetic nephropathy and extracellular matrix. J Histochem Cytochem. 2012; 60:976–986. PMID: 23103723.37. Battin M, Wouldes TA, Rowan J. Neurodevelopmental outcome in offspring born following gestational diabetes. In : Rajendram R, Preedy V, Patel V, editors. Nutrition and Diet in Maternal Diabetes: Nutrition and Health. Cham: Humana Press;2018. p. 341–354.38. Nobrega MA, Fleming S, Roman RJ, Shiozawa M, Schlick N, Lazar J, Jacob HJ. Initial characterization of a rat model of diabetic nephropathy. Diabetes. 2004; 53:735–742. PMID: 14988259.39. Gonzalez Suarez ML, Thomas DB, Barisoni L, Fornoni A. Diabetic nephropathy: is it time yet for routine kidney biopsy? World J Diabetes. 2013; 4:245–255. PMID: 24379914.40. Zini E, Benali S, Coppola L, Guscetti F, Ackermann M, Lutz TA, Reusch CE, Aresu L. Renal morphology in cats with diabetes mellitus. Vet Pathol. 2014; 51:1143–1150. PMID: 24565829.41. Friesen NT, Buchau AS, Schott-Ohly P, Lgssiar A, Gleichmann H. Generation of hydrogen peroxide and failure of antioxidative responses in pancreatic islets of male C57BL/6 mice are associated with diabetes induced by multiple low doses of streptozotocin. Diabetologia. 2004; 47:676–685. PMID: 15298345.42. Floege J, Eng E, Young BA, Johnson RJ. Factors involved in the regulation of mesangial cell proliferation in vitro and in vivo. Kidney Int Suppl. 1993; 39:S47–S54. PMID: 8468926.43. Kitching AR, Hutton HL. The players: cells involved in glomerular disease. Clin J Am Soc Nephrol. 2016; 11:1664–1674. PMID: 27073196.44. Weil EJ, Lemley KV, Yee B, Lovato T, Richardson M, Myers BD, Nelson RG. Podocyte detachment in type 2 diabetic nephropathy. Am J Nephrol. 2011; 33(Suppl 1):21–24. PMID: 21659731.45. Kumar D, Zimpelmann J, Robertson S, Burns KD. Tubular and interstitial cell apoptosis in the streptozotocin-diabetic rat kidney. Nephron Exp Nephrol. 2004; 96:e77–e88. PMID: 15056984.46. Inoki K, Mori H, Wang J, Suzuki T, Hong S, Yoshida S, Blattner SM, Ikenoue T, Ruegg MA, Hall MN, Kwiatkowski DJ, Rastaldi MP, Huber TB, Kretzler M, Holzman LB, Wiggins RC, Guan KL. mTORC1 activation in podocytes is a critical step in the development of diabetic nephropathy in mice. J Clin Invest. 2011; 121:2181–2196. PMID: 21606597.47. Gross ML, Amann K, Ritz E. Nephron number and renal risk in hypertension and diabetes. J Am Soc Nephrol. 2005; 16(Suppl 1):S27–S29. PMID: 15938029.48. Sison KT. Role of VEGF and VEGF receptors in the glomerulus [thesis]. Toronto: University of Toronto;2009.49. Crowther CA, Hiller JE, Moss JR, McPhee AJ, Jeffries WS, Robinson JS. Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial Group. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med. 2005; 352:2477–2486. PMID: 15951574.50. Moore LE, Briery CM, Clokey D, Martin RW, Williford NJ, Bofill JA, Morrison JC. Metformin and insulin in the management of gestational diabetes mellitus: preliminary results of a comparison. J Reprod Med. 2007; 52:1011–1015. PMID: 18161398.51. Morales AI, Detaille D, Prieto M, Puente A, Briones E, Arevalo M, Leverve X, Lopez-Novoa JM, El-Mir MY. Metformin prevents experimental gentamicin-induced nephropathy by a mitochondria-dependent pathway. Kidney Int. 2010; 77:861–869. PMID: 20164825.52. Tavafi M. Diabetic nephropathy and antioxidants. J Nephropathol. 2013; 2:20–27. PMID: 24475422.53. Gobe GC, Morais C, Vesey DA, Johnson DW. Use of high-dose erythropoietin for repair after injury: A comparison of outcomes in heart and kidney. J Nephropathol. 2013; 2:154–165. PMID: 24475445.54. Balsells M, García-Patterson A, Solà I, Roqué M, Gich I, Corcoy R. Glibenclamide, metformin, and insulin for the treatment of gestational diabetes: a systematic review and meta-analysis. BMJ. 2015; 350:h102. PMID: 25609400.55. Munshi S, Khandaker S. Evaluation of metformin versus insulin in the management of gestational diabetes mellitus: a prospective comparative study. Int J Reprod Contracept Obstet Gynecol. 2017; 3:357–361.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Proliferation of Cultured Vascular Smooth Muscle Cells(VSMCs) Obtained from Aortas of Insulin Dependent Diabetic Rats
- Effects of Polygonatum odoratum on In vivo Insulin Activity in Streptozotocin-Induced Diabetic Rats
- The Effects of Insulin Treatment on the Contractile Responses of the Seminal Vesicle in Streptozotocin-induced Diabetic Rats
- Effects of S-allylcysteine on Oxidative Stress in Streptozotocin-Induced Diabetic Rats
- Alteration of Nerve Growth Factor in the Penis of Rats with Streptozotocin-induced Diabetes
