The RAP Index during Intracranial Pressure Monitoring as a Clinical Guiding for Surgically Treated Aneurysmal Subarachnoid Hemorrhage: Consecutive Series of Single Surgeon
- Affiliations
-
- 1Department of Neurosurgery, Inje University Haeundae Paik Hospital, Busan, Korea. jheaj@hanmail.net
- KMID: 2449382
- DOI: http://doi.org/10.4266/acc.2019.00437
Abstract
- BACKGROUND
It is well known that assessing the RAP index along with intracranial pressure (ICP) monitoring in traumatic brain injury patients is helpful. We will discuss the usefulness of this assessment tool as a clinical guide for surgically treated poor grade aneurysmal subarachnoid hemorrhage (SAH).
METHODS
This retrospective study included 35 patients with aneurysmal SAH who presented with World Federation of Neurosurgical Societies (WFNS) grade V SAH and received surgical treatment from January 2013 to December 2018. Emergency surgical clipping, hematoma removal, extraventricular drainage, and if needed, wide decompressive craniectomy were combined as the proper surgical treatments. Outcomes were assessed based on in-hospital survival and the Glasgow outcome scale score at 14-day follow-up. We compared the mortality rate of two groups of seven patients: ICP monitoring only (n=5) and ICP monitoring combined with the RAP index (n=2).
RESULTS
The in-hospital 14-day mortality rate by brain lesion was 48.5% (n=17). Seven patients had real-time ICP monitoring. Before 2018, three of five patients with poor WFNS grade who received real-time ICP monitoring only died. There were no deaths in the group of two patients receiving real-time ICP monitoring and the RAP index.
CONCLUSIONS
Our data indicate that combining the RAP index and ICP monitoring can be used as markers for critical intracranial physiological parameters in poor grade WFNS patients.
MeSH Terms
Figure
-

Figure 1. (A) Illustration wave graph of the intracranial pressure (ICP) and amplitude (AMP). Rising ICP leads the AMP increase. AMP starts at 0 and reaches peak at the critical ICP (blue arrow) and finally back to 0. (B) Illustration graph of the ICP and AMP. The RAP index and ICP are initially 0, first black arrow (cerebral autoregulation is not functioning). The RAP index is positive to the critical ICP (blue arrow). Beyond the critical ICP the RAP index tuned negative and finally goes back to 0 again, second black arrow (cerebral autoregulation is broken). (C) Illustration graph of the ICP and cumulative sum of AMP. As ICP rises, the cumulative sum of AMP resembles exactly the Starling pressure-volume curve. The steepest slope point on the curve is the critical ICP (blue arrow).
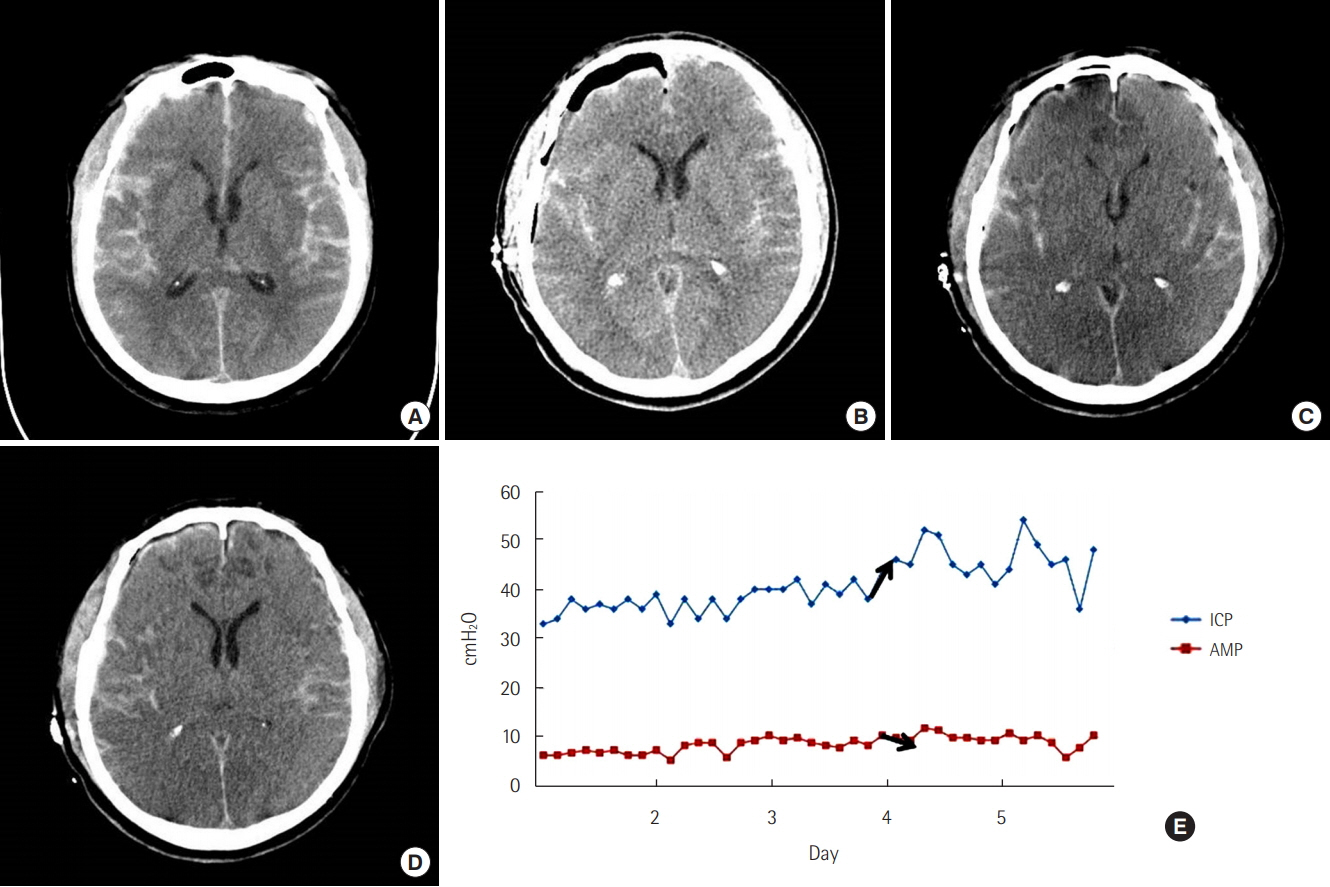
Figure 2. A 51-year-old woman presented as comatose due to rupture of a right middle cerebral artery aneurysm bifurcation aneurysm. (A) A preoperative computed tomography (CT) scan shows subarachnoid hemorrhage and a small amount of subdural hematoma. (B) Immediate postoperative CT scan shows craniotomy state and pneumocephalus. (C) The 4th postoperative day’s CT scan shows severe brain swelling and diffuse low-density lesion. (D) The 7th postoperative day’s CT scan shows slightly improving brain swelling and a nonprogressing low-density lesion. (E) Illustration graph of the intracranial pressure (ICP) and amplitude (AMP) of the patient. On the 2nd postoperative day, the ICP was still over 30 cmH2O but the AMP was not significantly changed. However, on the 4th postoperative day, the ICP rose over 40 cmH2O and AMP decreased (black arrows). We thought the RAP index was changing toward a negative aspect and the patient had reached critical ICP.
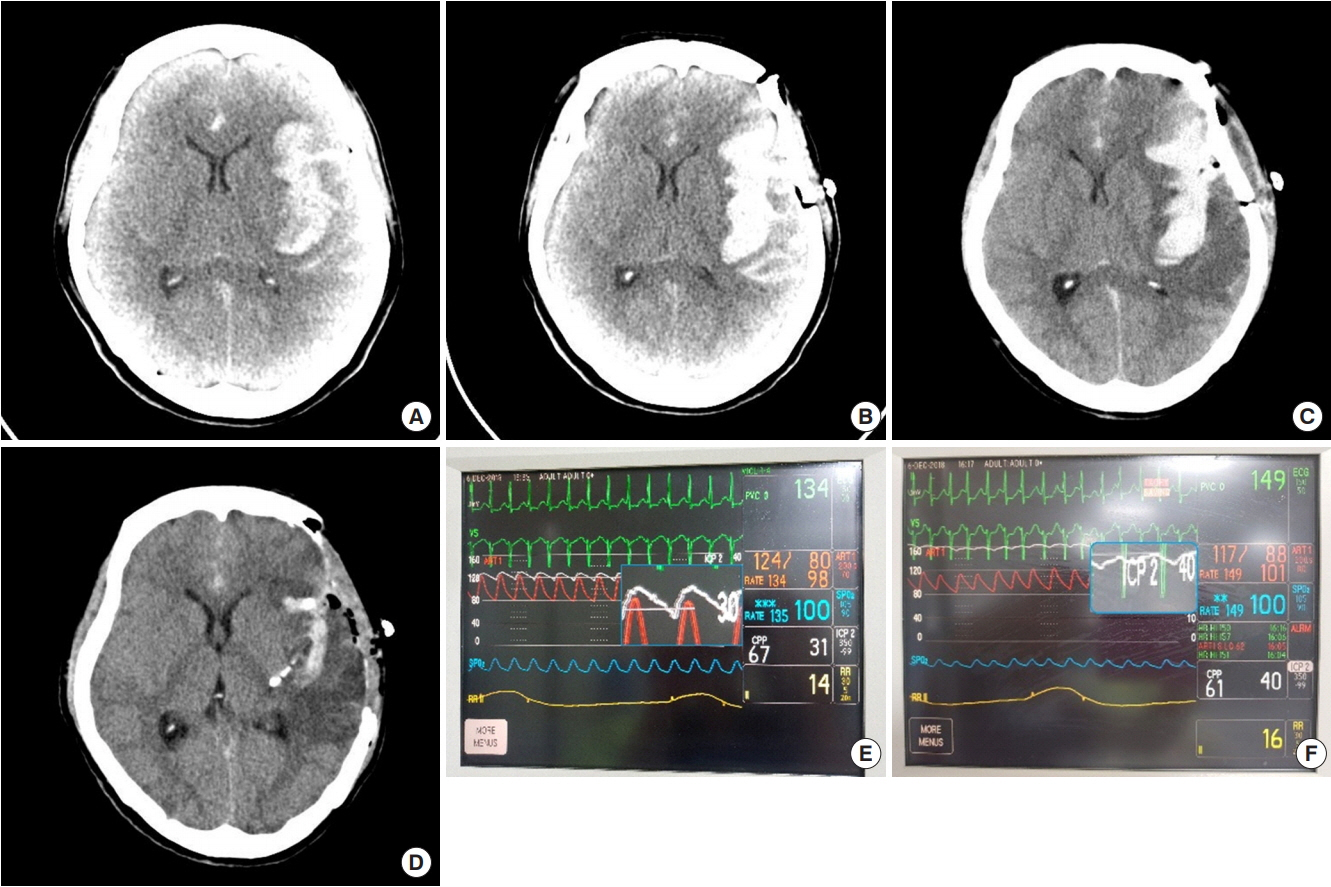
Figure 3. A 48-year-old man presented in a semicomatose state due to the rupture of a left middle cerebral artery aneurysm bifurcation aneurysm. (A) A preoperative computed tomography (CT) scan shows subarachnoid hemorrhage (SAH) and a thick sylvian hematoma. (B) Immediate postoperative CT scan shows craniotomy and remnant SAHs. (C) The 2nd postoperative day’s CT scan shows an increased lowdensity lesion around the sylvian hematoma. (D) After the second operation, the CT scan shows craniectomy state and decreased brain swelling and sylvian hematoma. (E) Intracranial pressure (ICP) monitoring using a sylvian drainage catheter connected to an arterial pressure monitor kit. (F) On the 2nd postoperative day, ICP rose to 40 cmH2O from 30 cmH2O and amplitude decreased remarkably. The RAP index just changed negatively implying the patient has reached a critical ICP (blue square, white line).
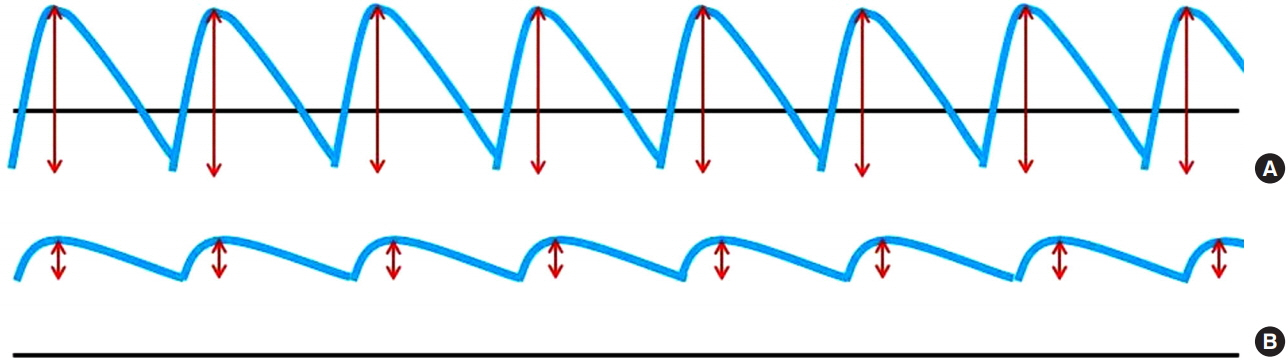
Figure 4. Intracranial pressure (ICP) monitoring waves depicting amplitude (AMP) changes from a positive RAP index to a negative one as the patient ICP fluctuates. (A) Red lines illustrate the AMP of the ICP wave (blue line) and the average of the AMPs gives the ICP mean pulse AMP. (B) Decreased AMP implies the RAP index inversion from the positive to the negative which prompted additional management for the patient just reaching critical ICP.
Reference
-
1. Hoogmoed J, Coert BA, van den Berg R, Roos YB, Horn J, Vandertop WP, et al. Early treatment decisions in poor-grade patients with subarachnoid hemorrhage. World Neurosurg. 2018; 119:e568–73.
Article2. Zheng K, Zhao B, Tan XX, Li ZQ, Xiong Y, Zhong M, et al. Comparison of aggressive surgical treatment and palliative treatment in elderly patients with poor-grade intracranial aneurysmal subarachnoid hemorrhage. Biomed Res Int. 2018; 2018:5818937.
Article3. Aguilar-Aguilar G, García-Raimundo M, Talamantes-Escribá F, Maruenda-Paulino A, Badenes-Catalá R, Belda-Nacher FJ. Intraparenchymal cerebral hematoma following the insertion of a catheter for monitoring intracranial pressure. Rev Esp Anestesiol Reanim. 1999; 46:45–6.4. Czosnyka M, Steiner L, Balestreri M, Schmidt E, Smielewski P, Hutchinson PJ, et al. Concept of “true ICP” in monitoring and prognostication in head trauma. Acta Neurochir Suppl. 2005; 95:341–4.
Article5. Varsos GV, Kasprowicz M, Smielewski P, Czosnyka M. Modelbased indices describing cerebrovascular dynamics. Neurocrit Care. 2014; 20:142–57.
Article6. Powers WJ. Cerebral hemodynamics in ischemic cerebrovascular disease. Ann Neurol. 1991; 29:231–40.
Article7. Momjian-Mayor I, Baron JC. The pathophysiology of watershed infarction in internal carotid artery disease: review of cerebral perfusion studies. Stroke. 2005; 36:567–77.8. Steiner LA, Andrews PJ. Monitoring the injured brain: ICP and CBF. Br J Anaesth. 2006; 97:26–38.
Article9. Duschek S, Schandry R. Reduced brain perfusion and cognitive performance due to constitutional hypotension. Clin Auton Res. 2007; 17:69–76.
Article10. Kim DJ, Czosnyka Z, Keong N, Radolovich DK, Smielewski P, Sutcliffe MP, et al. Index of cerebrospinal compensatory reserve in hydrocephalus. Neurosurgery. 2009; 64:494–501.
Article11. Hall A, O’Kane R. The best marker for guiding the clinical management of patients with raised intracranial pressure-the RAP index or the mean pulse amplitude? Acta Neurochir (Wien). 2016; 158:1997–2009.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hemodynamics of Poor-grade Subarachnoid Hemorrhage
- Evaluation of Subarachnoid Hemorrhage due to Aneurysmal Rupture and Cerebral Vasospasm by CT
- Nimodipine Treatment after Aneurysmal Subarachnoid Hemorrhage and Operation
- Clinical Trial of Nimodipine in Patients with Aneurysmal Subarachnoid Hemorrhage
- Comparison of Clinical Usefulness of Lumboperitoneal Shunt with Ventriculoperitoneal Shunt for Treating Chronic Hydrocephalus in Ruptured Intracranial Aneurysm
