Combination Therapy of Angiotherapy, Radiation Therapy, and Radiofrequency Ablation for Pulmonary Metastasis of Hepatocellular Carcinoma Accompanied by Nontuberculous Mycobacteria
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. bik.kim@samsung.com
- 2Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2448282
- DOI: http://doi.org/10.17998/jlc.19.1.79
Abstract
- With the advances in hepatocellular carcinoma (HCC) treatment, the lung metastasis of HCC is becoming increasingly important. In treating the lung metastasis of HCC, a multidisciplinary approach can lead to better results than systemic chemotherapy alone. Here, we report on a patient who presented with pulmonary masses, while the HCC was being controlled in the abdominal cavity. The presence of nontuberculous mycobacteria was identified during the diagnosis of the pulmonary masses. The pulmonary metastases of HCC were treated with a combination of angiotherapy, radiation therapy, and radiofrequency ablation. The patient showed a satisfactory progress with this multidisciplinary localized treatment. We report the clinical progress and review the recent literature regarding the treatment of pulmonary metastasis without intrahepatic HCC herein.
MeSH Terms
Figure
-
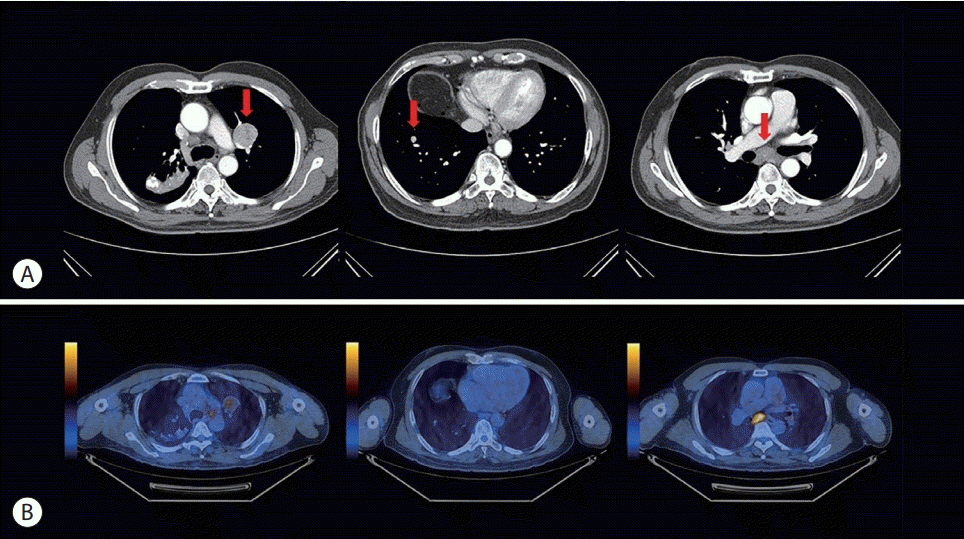
Figure 1. CECT scan revealing well-defined, round masses (35 mm in the LUL and 10 mm in the RLL, each is marked with an arrow in the left and middle images) and enlarged subcarinal lymph node (arrow in the right image) with faint central calcification. (B) PET-CT performed one week after CECT showing increased FDG uptakes in the LUL mass and subcarinal lymph node. CECT, contrastenhanced computed tomography; LUL, left upper lobe; RLL, right lower lobe; PET-CT, positron emission tomography-computed tomography; FDG, fluorodeoxyglucose.
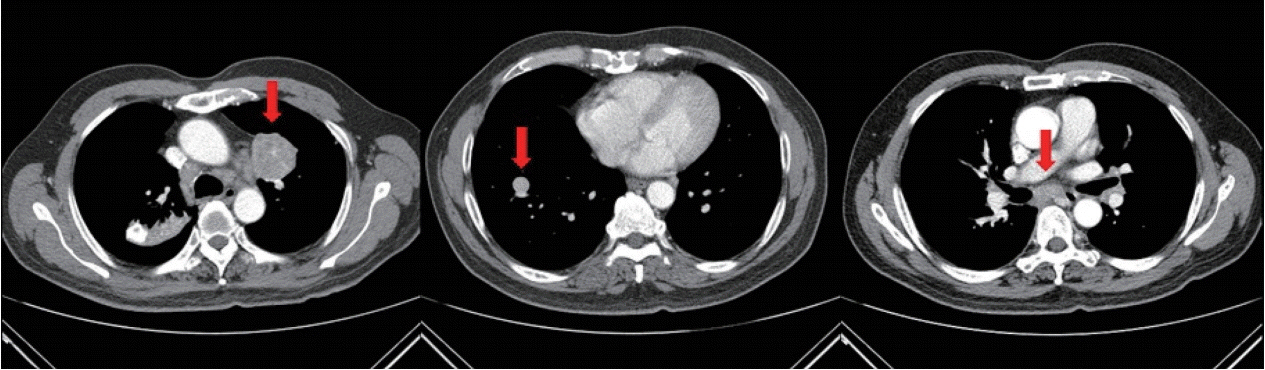
Figure 2. Follow-up CECT showing interval enlarged LUL mass (arrow in the left image) with heterogeneous contrast enhancement and internal lower densities, as well as an interval enlarged RLL mass (arrow in the middle image). Both lung masses appear suggestive of pulmonary metastasis. When compared with the initial CECT scan, interval increases in the sizes of mediastinal lymph nodes (arrow in the right image) can be seen. CECT, contrast-enhanced computed tomography; LUL, left upper lobe; RLL, right lower lobe.

Figure 3. Histopathology of the pulmonary metastasis. (A) H&E staining of the lung mass showing metastatic hepatocellular carcinoma (original magnification, ×200). (B) Tumor cells appear positive for hepatocyte-specific antigen (original magnification, ×200). H&E, hematoxylin and eosin.
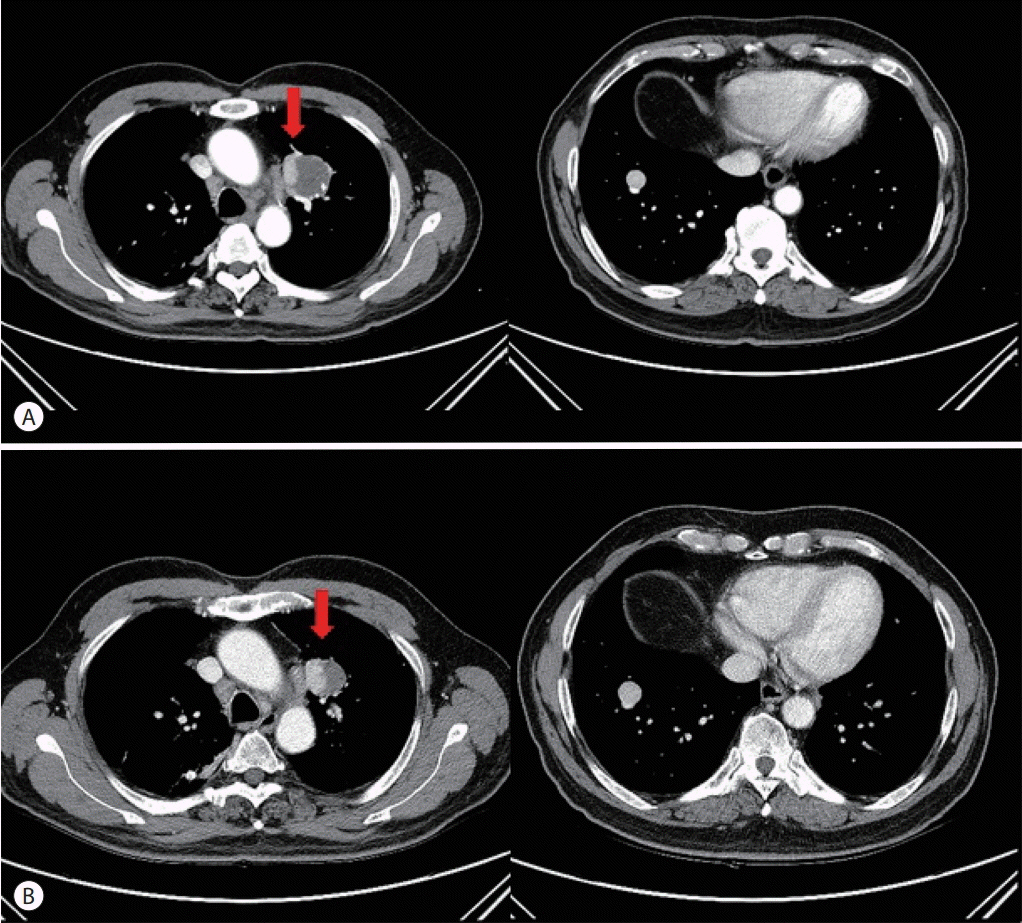
Figure 4. (A) CECT performed one month after BAE showing that the size of the LUL mass (arrow) decreased from 44 mm to 40 mm. However, there an enhancing portion remained, suggesting viable foci. (B) CECT performed one month after radiotherapy showing that, in the LUL mass (arrow), the enhancing lesion elongated at the medial aspect. The size of the RLL mass increased from 15 mm to 17 mm. CECT, contrast-enhanced computed tomography; BAE, bronchial artery embolization; LUL, left upper lobe; RLL, right lower lobe.
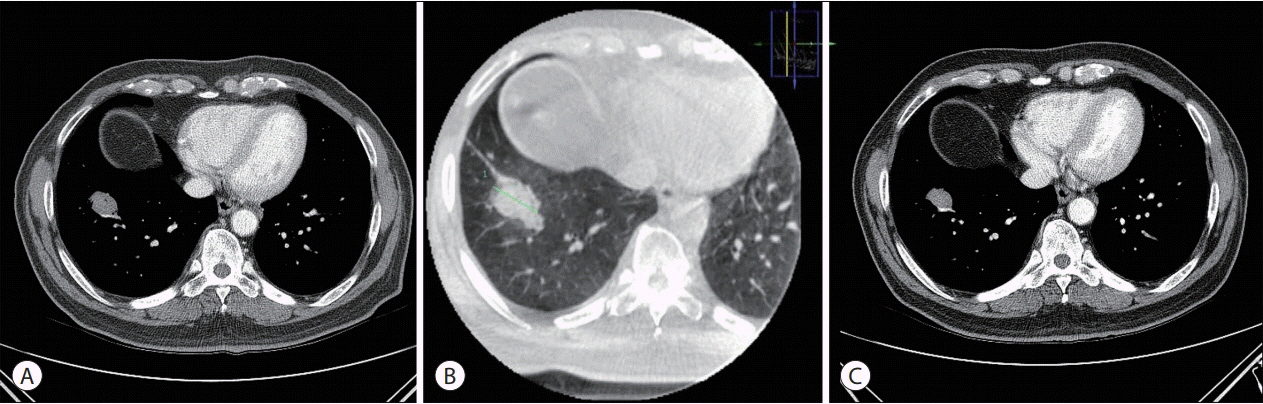
Figure 5. (A) The left CECT scan was performed one month after RFA. Immediate follow-up CECT revealing an increase in the size of the RLL nodule. (B) Cone-beam CT was performed during the RFA procedure. Ground-glass opacity formed around the RLL mass. (C) The right CECT scan was performed three months after RFA. The size of the RLL mass decreased, and there was no viable portion in the mass. CECT, contrast-enhanced computed tomography; RFA, radiofrequency ablation; RLL, right lower lobe; CT, computed tomography.
Reference
-
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424.2. Kim BH, Park JW. Epidemiology of liver cancer in South Korea. Clin Mol Hepatol. 2018; 24:1–9.3. Chan KM, Yu MC, Wu TJ, Lee CF, Chen TC, Lee WC, et al. Efficacy of surgical resection in management of isolated extrahepatic metastases of hepatocellular carcinoma. World J Gastroenterol. 2009; 15:5481–5488.4. Aramaki M, Kawano K, Kai T, Yokoyama H, Morii Y, Sasaki A, et al. Treatment for extrahepatic metastasis of hepatocellular carcinoma following successful hepatic resection. Hepatogastroenterology. 1999; 46:2931–2934.5. Hiraki T, Gobara H, Takemoto M, Mimura H, Mukai T, Himei K, et al. Percutaneous radiofrequency ablation combined with previous bronchial arterial chemoembolization and followed by radiation therapy for pulmonary metastasis from hepatocellular carcinoma. J Vasc Interv Radiol. 2006; 17:1189–1193.6. Llovet JM, Villanueva A, Lachenmayer A, Finn RS. Advances in targeted therapies for hepatocellular carcinoma in the genomic era. Nat Rev Clin Oncol. 2015; 12:408–424.7. Lee SJ, Lim SY, Yoo TK, Kim SK, Kim YG, Lee HJ, et al. A case of synchronous lung squamous cell carcinoma and diffuse large B-cell lymphoma. Korean J Med. 2018; 93:300–305.8. Kee SJ, Suh SP. Increasing burden of nontuberculous mycobacteria in Korea. J Korean Med Sci. 2017; 32:1215–1216.9. Petrella F, Diotti C, Rimessi A, Spaggiari L. Pulmonary metastasectomy: an overview. J Thorac Dis. 2017; 9(Suppl 12):S1291–S1298.10. Guy J, Kelley RK, Roberts J, Kerlan R, Yao F, Terrault N. Multidisciplinary management of hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2012; 10:354–362.11. Mehta AS, Ahmed O, Jilani D, Zangan S, Lorenz J, Funaki B, et al. Bronchial artery embolization for malignant hemoptysis: a single institutional experience. J Thorac Dis. 2015; 7:1406–1413.12. Kishore S, Friedman T, Madoff DC. Update on embolization therapies for hepatocellular carcinoma. Curr Oncol Rep. 2017; 19:40.13. Ryoo HM. Management of pulmonary metastasis. Korean J Med. 2011; 81:289–299.14. Hachisuka Y, Uomoto M, Fujisawa T, Mogami H. First reported case of lung metastasis from hepatocellular carcinoma successfully treated by ultrasound-guided radiofrequency ablation using ultrasonic contrast agent. Gan To Kagaku Ryoho. 2009; 36:2657–2659.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Role of Combination of Transarterial Chemoebolization and Radiofrequency Ablation for Hepatocellular Carcinoma Treatment
- Is Percutaneous Ethanol Injection Therapy Still Effective for Hepatocellular Carcinoma in the Era of Radiofrequency Ablation?
- Current status and future of radiofrequency ablation for hepatocellular carcinoma
- Microwave thermosphere versus radiofrequency ablation for hepatocellular carcinoma: Are we approaching the time to end the debate?
- Radiofrequency Thermal Ablation of Hepatocellular Carcinomas
