Radiofrequency Thermal Ablation of Hepatocellular Carcinomas
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hklim@smc.samsung.co.kr
- KMID: 1378942
- DOI: http://doi.org/10.3348/kjr.2000.1.4.175
Abstract
- Although surgical resection remains the best option as potentially curative therapy for hepatocellular carcinoma, radiofrequency thermal ablation has begun to receive much attention as an effective minimally invasive technique for the local control of unresectable malignant hepatic tumors. Most recent radiofrequency devices equipped with a powerful generator and larger needle electrode permit larger thermal lesions, up to 5 cm in diameter, with a single ablation. In this article, the author reviews the technical developments and early clinical results obtained with radiofrequency ablation techniques.
MeSH Terms
Figure
-
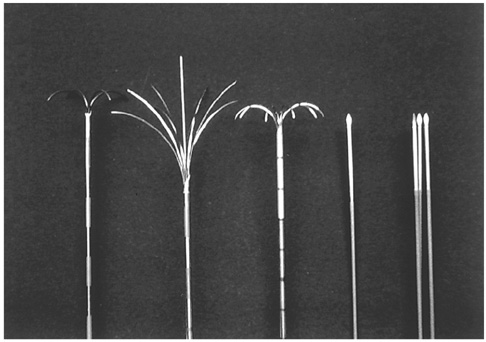
Fig. 1 Radiofrequency needle electrodes of varying design manufactured by three different companies. The first three needle electrodes, 15-gauge in external diameter and insulated except for 0.6-1 cm of their tip, have 4, 9, or 10 retractable hook-like prongs which serve as active electrodes during RF ablation. The fourth and fifth have a single 17-gauge straight-tip and triple-cluster electrodes, internally cooled with chilled saline solution during ablation. The needles have active exposed tips 2-4 cm in length
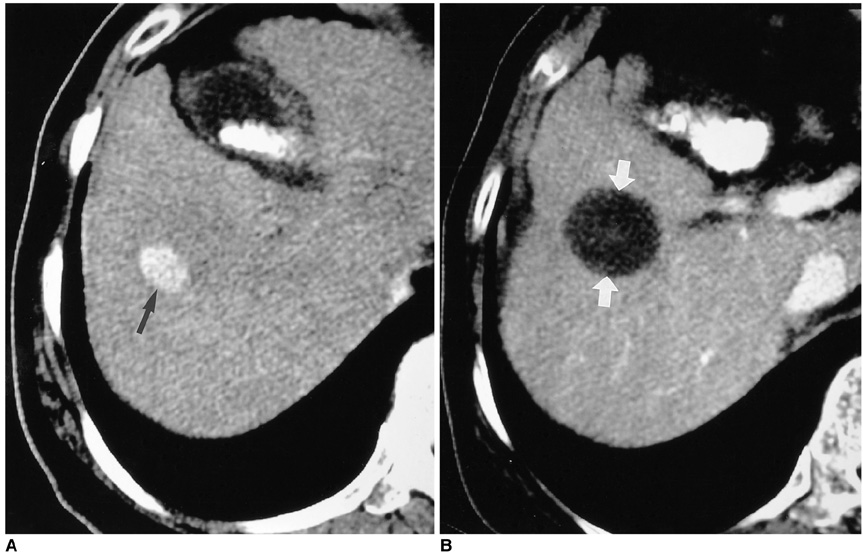
Fig. 2 HCC located in the mid-zone of the liver surrounded by normal hepatic tissue in a 62-year-old man. A. Transverse helical CT scan obtained during the hepatic arterial phase prior to RF ablation shows a 2.5-cm HCC (arrow), with homogenous contrast enhancement in liver segment 5. B. Transverse helical CT scan obtained one month after RF ablation depicts a round ablated area of low attenuation (arrows), representing complete necrosis of the tumor. Note that the ablated area covers the entire tumor and the cuff of surrounding normal hepatic tissue.
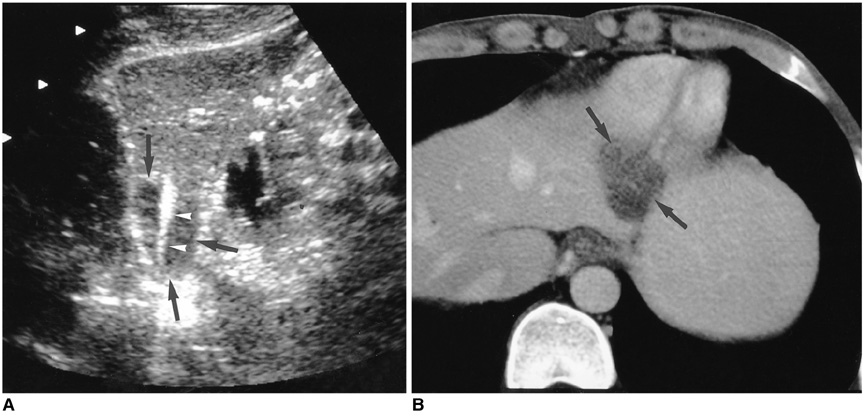
Fig. 3 HCC in a 45-year-old man. A. Longitudinal US scan of left hepatic lobe shows a 2.8-cm low echogenic HCC (arrows) which is fusiform in shape. The mass abuts on both liver capsules. Note the 3-cm active tip (arrowheads) of the straight cooled-tip electrode, which conforms to the shape of the mass. A single ablation lasted for 12 minutes. B. Portal-phase CT scan obtained 30 minutes after RF ablation reveals the presence of an oval low-attenuating lesion (arrows), with absence of contrast enhancement within the ablated area. This indicates complete necrosis.

Fig. 4 HCC in a 57-year-old man. A. Hepatic arterial-phase CT scan depicts a 4-cm HCC (arrows) in the subcapsular area of the right hepatic lobe, which shows an outward bulge. Using a 3-cm expandable needle electrode, four ablations were performed. The deep portion of the mass was treated first, and then the exophytic portion. B. Portal-phase CT scan obtained 13 months after RF ablation shows an ablated lesion (arrows) with no contrast enhancement, indicating complete necrosis.
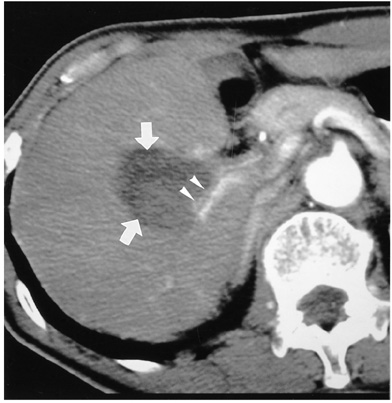
Fig. 5 Hepatic arterial-phase CT scan obtained 1 month after RF ablation of a 4-cm HCC surrounded by large branches of the hepatic artery and portal vein shows a low attenuating ablated lesion (arrows) near the hepatic hilum. Although the tumor has become mostly necrotic, thin enhancing viable tumor (arrowheads) remains along the posterior branch of the right hepatic artery.
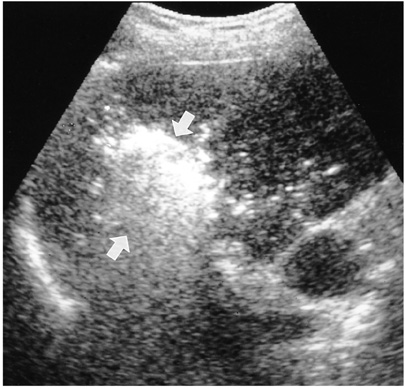
Fig. 6 Oblique US scan of the liver obtained during RF ablation shows an echogenic ablated lesion (arrows), the result of numerous microbubbles produced by thermal ablation.
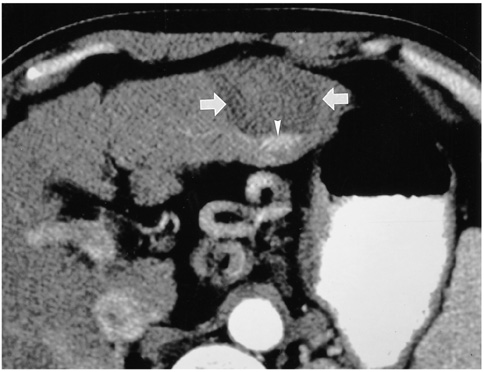
Fig. 7 Hepatic arterial-phase CT scan obtained one month after RF ablation of a 4-cm HCC in the left hepatic lobe reveals the presence of a round low-attenuating lesion (arrows). Note the focal contrast enhancement (arrowhead) in the posterior aspect of the ablated lesion, indicative of viable untreated tumor. Additional RF ablation was subsequently performed.
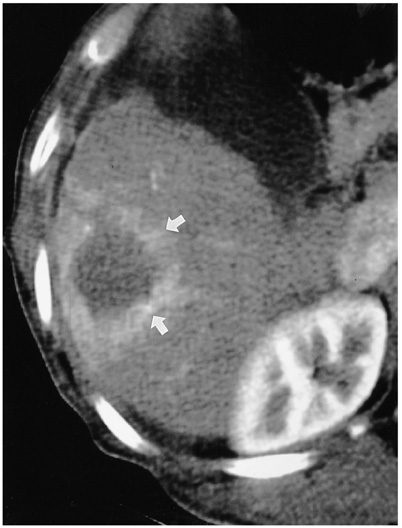
Fig. 8 Reactive hyperemia revealed by immediate post-treatment CT. Hepatic arterial-phase CT scan obtained 30 minutes after RF ablation shows uniform rim-like contrast enhancement (arrows) around the ablated lesion, a phenomenon frequently occurring immediately after RF ablation and usually resolving prior to follow-up CT at one month.
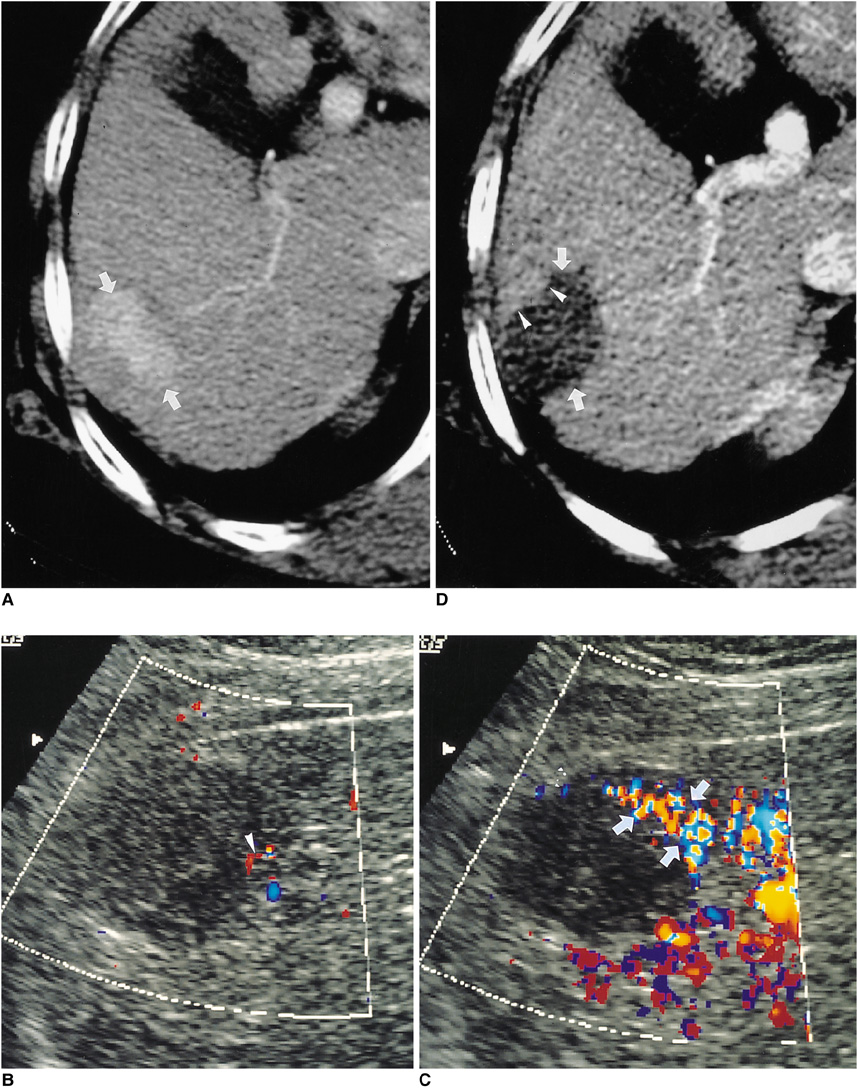
Fig. 9 HCC in a 67-year-old woman. A. Hepatic arterial-phase CT scan shows an oval enhancing HCC (arrows), 4 cm in its greatest diameter, at the periphery of the right hepatic lobe. B. Unenhanced oblique power Doppler US scan obtained 18 hours after RF ablation shows a subtle flow signal (arrowhead) in the antero-superior aspect of the ablated lesion. C. Contrast-enhanced oblique power Doppler US scan obtained immediately after B, above, shows peripheral flow signals (arrows) within the anterior aspect of the RF-ablated lesion, representing residual tumor. The residual flow signals seen on this contrast-enhanced scan are better appreciated than on nonenhanced power Doppler US scan. D. Hepatic arterial-phase CT scan obtained 2 hours after RF ablation shows focal nodular contrast enhancement (arrowheads), indicative of residual tumor, in the anterior aspect of the ablated lesion (arrows). The enhanced area corresponds to that in which residual flow signals are present in the image described in C, above.
Reference
-
1. Colombo M. Hepatocellular carcinoma. J Hepatol. 1992. 15:225–236.2. Tsuzuki T, Sugioka A, Ueda M. Hepatic resection for hepatocellular carcinoma. Surgery. 1990. 107:511–520.3. Liver Cancer Study Group of Japan. Primary liver cancer in Japan: clinicopathologic features and results of surgical treatment. Ann Surg. 1990. 211:277–284.4. Farmer DG, Rosove MH, Shaked A, Busuttil RW. Current treatment modalities for hepatocellular carcinoma. Ann Surg. 1994. 219:236–247.5. Livraghi T, Bolondi L, Lazzaroni S, et al. Percutaneous ethanol injection in the treatment of hepatocellular carcinoma in cirrhosis: a study in 207 patients. Cancer. 1992. 69:925–929.6. Honda N, Guo Q, Uchida H, Ohishi H, Hiasa Y. Percutaneous hot saline injection therapy for hepatic tumors: an alternative to percutaneous ethanol injection therapy. Radiology. 1994. 190:53–57.7. Amin Z, Donald JJ, Masters A, et al. Hepatic metastases: interstitial laser photocoagulation with real-time sonography monitoring and dynamic CT evaluation of treatment. Radiology. 1993. 187:339–347.8. Murakami R, Yoshimatsu S, Yamashita Y, Matsukawa T, Takahashi M, Sagara K. Treatment of hepatocellular carcinoma: value of percutaneous microwave coagulation. AJR. 1995. 164:1159–1164.9. McGahan JP, Browning PD, Brock JM, Tesluk H. Hepatic ablation using radiofrequency electrocautery. Invest Radiol. 1990. 25:264–270.10. Goldberg SN, Gazelle GS, Dawson SI, et al. Tissue ablation with radiofrequency using multiprobe arrays. Acad Radiol. 1995. 2:670–674.11. Livraghi T, Goldberg SN, Monti F, et al. Saline-enhanced radiofrequency tissue ablation in the treatment of liver metastasis. Radiology. 1997. 202:205–210.12. Rossi S, Buscarini E, Garbagnati F, et al. Percutaneous treatment of small hepatic tumors by an expandable RF needle electrode. AJR. 1998. 170:1015–1022.13. Curley SA, Izzo F, Delrio P, et al. Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg. 1999. 230:1–8.14. Solbiati L, Goldberg SN, Ierace T, et al. Hepatic metastases: percutaneous radio-frequency ablation with cooled-tip electrodes. Radiology. 1997. 205:367–373.15. Rossi S, Di Stasi M, Buscarini E, et al. Percutaneous RF interstitial thermal ablation in the treatment of hepatic cancer. AJR. 1996. 167:759–768.16. Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Solbiati L, Gazelle GS. Small hepatocellular carcinoma: treatment with radio-frequency ablation versus ethanol injection. Radiology. 1999. 210:655–661.17. Livraghi T, Goldberg SN, Lazzaroni S, et al. Hepatocellular carcinoma: radio-frequency ablation of medium and large lesions. Radiology. 2000. 214:761–768.18. Goldberg SN, Solbiati L, Hahn PF. Large-volume tissue ablation with radiofrequency by using a clustered, internally cooled electrode: laboratory and clinical experience in liver metastases. Radiology. 1998. 209:371–379.19. Choi D, Lim HK, Park JM, et al. An experimental study on hepatic ablation using an expandable radiofrequency needle electrode. J of Korean Radiol Soc. 1999. 41:1127–1132.20. Choi D, Lim HK, Kim SH, et al. Radiofrequency ablation of small heaptocellular carcinoma: early experience of efficacy and safety. J of Korean Radiol Soc. 2000. 42:743–749.21. Hornback NB. Historical aspects of hyperthermia in cancer therapy. Radiol Clin North Am. 1989. 27:481–488.22. Coley WB. The treatment of malignant tumors by repeated innoculations of erysipelas, with a report of ten original cases. Am J Med Sci. 1893. 105:487–492.23. Rosomoff Hl, Carroll F, Brown J, Sheptak T. Percutaneous radiofrequency cervical cordotomy technique. J Neurosurgery. 1965. 23:639–644.24. LeVenn HH, Ahmed N, Piccone VA, Shugaar S, Falk G. Radiofrequency therapy: clinical experience. Ann N Y Acad Sci. 1980. 335:362–371.25. Seki T, Wakabayashi M, Nakagawa T, et al. Ultrasonically guided percutaneous microwave coagulation therapy for small hepatocellular carcinoma. Cancer. 1994. 74:817–825.26. Dickson JA, Calderwood SK. Temperature range and selective sensitivity of tumors to hyperthermia: a critical review. Ann N Y Acad Sci. 1980. 335:180–205.27. Hill RP, Hunt JW. Tannock IF, Hill RF, editors. Hyperthermia. The Basic Science of Oncology. 1987. New York: Pergamon Press;337–357.28. Allain JC, LeLouis M, Bailey AJ, Delaunay A. Isometric tension developed during heating of collagen tissues: relationship with collagen cross-linking. Biochimica et Biophysica Acta. 1978. 533:147–155.29. Haines DE, Verow AF. Observations on the electrode-tissue interface temperature and effect on electrical impendance during radiofrequency ablation of ventricular myocardium. Circ. 1990. 82:1034–1038.30. Goldberg SN, Hahn PF, Tanabe KK, et al. Percutaneous radiofrequency tissue ablation: does perfusion-mediated tissue cooling limit coagulation necrosis? J Vasc Interv Radiol. 1998. 9:101–111.31. Patterson EJ, Scudamore CH, Owen DA, Nagy AG, Buczkowski AK. Radiofrequency ablation of porcine liver in vivo: effects of blood flow and treatement time on lesion size. Annals of Surgery. 1998. 227:559–565.32. Goldberg SN, Hahn PF, Halpern EF, Fogle RM, Gazelle GS. Radio-frequency tissue ablation: effect of pharmacologic modulation of blood flow on coagulation diameter. Radiology. 1998. 209:761–767.33. Goldberg SN, Gazelle GS, Solbiati L, et al. Ablation of liver tumors using percutaneous RF therapy. AJR. 1998. 170:1023–1028.34. Choi D, Lim HK, Lee WJ, et al. Evaluation of therapeutic response in hepatocellular carcinoma treated with percutaneous radio-frequency ablation: usefulness of power Doppler US with a microbubble contrast agent-preliminary results. Radiology. 2000. 217:558–563.35. Lim HK. Radiofrequency ablation of hepatocellular carcinoma. Proceedings of the 4th Asian Pacific Congress of Cardiovascular and Interventional Radiology. 2000. 120–122.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Completely Ablated Hepatocellular Carcinoma by Percutaneous Radiofrequency Thermal Ablation
- Skin Burn after Laparoscopic Radiofrequency Thermal Ablation for Uterine Myoma : A case report
- Radiofrequency Thermal Ablation of Hepatocellular Carcinoma
- Microwave thermosphere versus radiofrequency ablation for hepatocellular carcinoma: Are we approaching the time to end the debate?
- Chemoembolization combined with radiofrequency ablation is the best option for the local treatment of early hepatocellular carcinoma?
