Emerging Role of Hepatobiliary Magnetic Resonance Contrast Media and Contrast-Enhanced Ultrasound for Noninvasive Diagnosis of Hepatocellular Carcinoma: Emphasis on Recent Updates in Major Guidelines
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Seoul, Korea. jmlshy2000@gmail.com
- 2Department of Radiology, Seoul National University Hospital, Seoul, Korea.
- 3Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea.
- KMID: 2447066
- DOI: http://doi.org/10.3348/kjr.2018.0450
Abstract
- Hepatocellular carcinoma (HCC) can be noninvasively diagnosed on the basis of its characteristic imaging findings of arterial phase enhancement and portal/delayed "washout" on computed tomography (CT) and magnetic resonance imaging (MRI) in cirrhotic patients. However, different specific diagnostic criteria have been proposed by several countries and major academic societies. In 2018, major guideline updates were proposed by the Association for the Study of Liver Diseases, European Association for the Study of the Liver (EASL), Korean Liver Cancer Association and National Cancer Center (KLCA-NCC) of Korea. In addition to dynamic CT and MRI using extracellular contrast media, these new guidelines now include magnetic resonance imaging (MRI) using hepatobiliary contrast media as the first-line diagnostic test, while the KLCA-NCC and EASL guidelines also include contrast-enhanced ultrasound (CEUS) as the second-line diagnostic test. Therefore, hepatobiliary MR contrast media and CEUS will be increasingly used for the noninvasive diagnosis and staging of HCC. In this review, we discuss the emerging role of hepatobiliary phase MRI and CEUS for the diagnosis of HCC and also review the changes in the HCC diagnostic criteria in major guidelines, including the KLCA-NCC practice guidelines version 2018. In addition, we aimed to pay particular attention to some remaining issues in the noninvasive diagnosis of HCC.
MeSH Terms
Figure
-
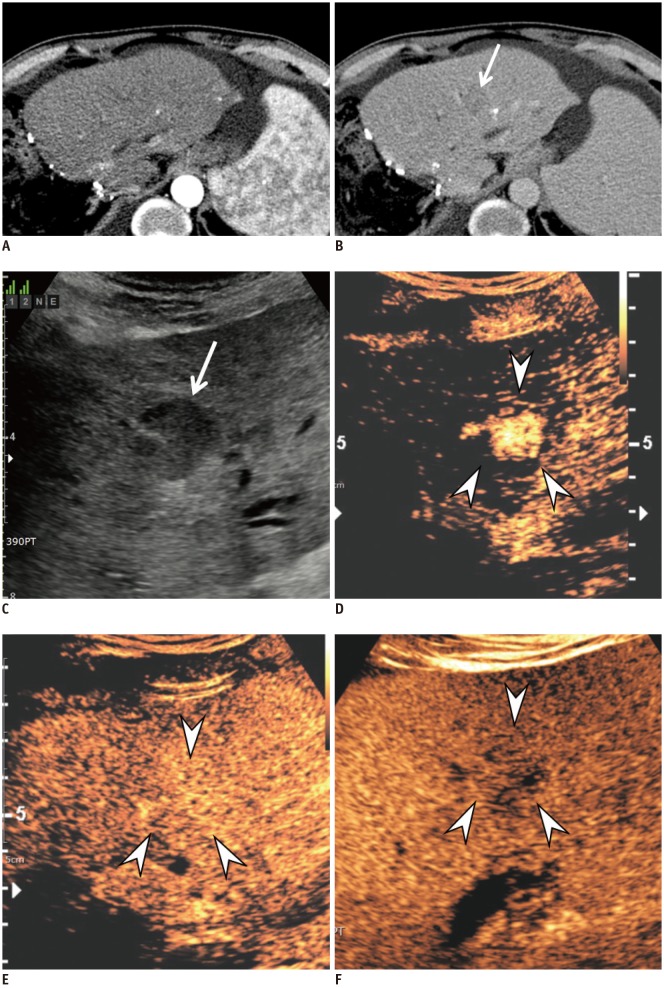
Fig. 1 Typical CEUS features of HCC in 60-year-old man with history of right hemihepatectomy for HCC.On arterial (A) and delayed (B) phases of CT, 2.3-cm subtle low-attenuated nodule (arrow) is visible only in delayed phase at left lateral segment of liver. Nodule (arrow) shows low echogenicity on gray-scale US (C). On CEUS, nodule (arrowheads) shows hyperenhancement in arterial phase (25 seconds after contrast injection) (D), isoechogenicity in portal phase (45 seconds) (E), and mild washout occurring only in late phase (200 seconds) (F), compatible with LI-RADS 5. CEUS = contrast-enhanced ultrasound, CT = computed tomography, HCC = hepatocellular carcinoma, LI-RADS = Liver Imaging Reporting and Data System, US = ultrasound
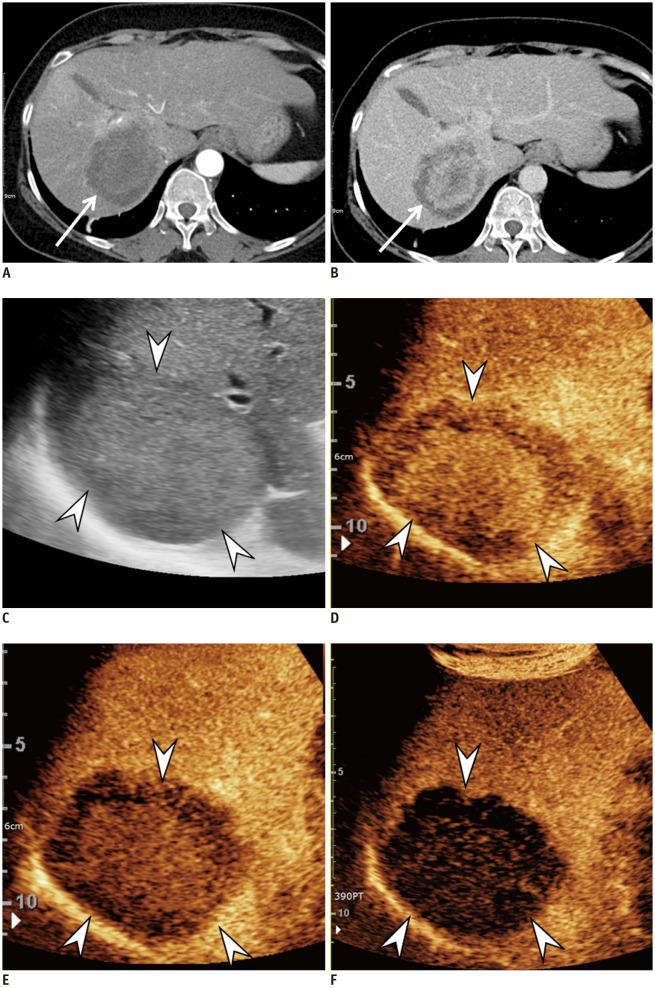
Fig. 2 Typical CEUS findings of cholangiocarcinoma in 57-year-old woman with CHB viral infection.On arterial (A) and portal (B) phases of CT, 8-cm low-attenuated mass (arrows) is seen with equivocal hyperenhancement in arterial phase and central hyperenhancement with peripheral low attenuation in 3-minute delayed phase at right lobe of liver. Mass (arrowheads) shows isoechogenicity on gray-scale US (C). On CEUS, mass (arrowheads) shows heterogeneous central hyperenhancement in arterial phase (20 seconds after contrast injection) (D), marked washout in both portal (60 seconds) (E) and late (180 seconds) (F) phases, compatible with LI-RADS-M. Lesion was confirmed as cholangiocarcinoma via biopsy. CHB = chronic hepatitis B
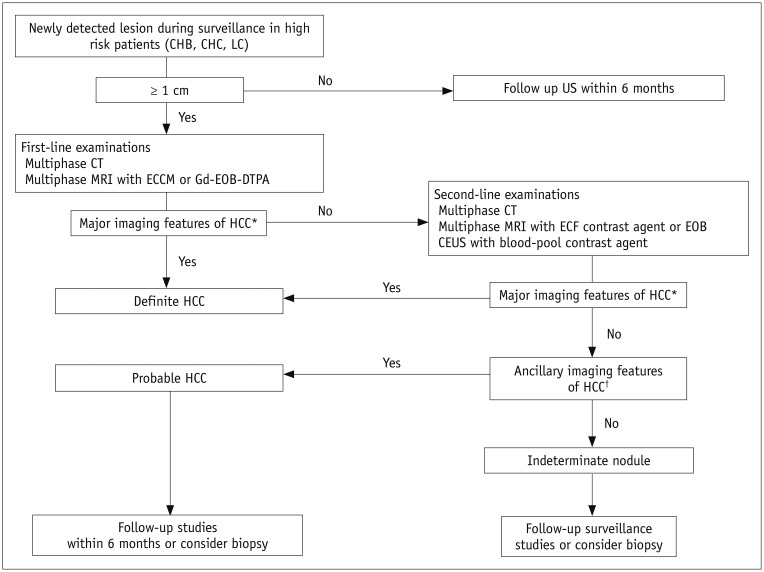
Fig. 3 Diagnostic algorithm for suspected HCC using new KLCA-NCC practice guidelines.*Major imaging features of HCC include arterial hyperenhancement and washout appearance during portal venous, delayed, or HBP on multiphasic CT or MRI using extracellular contrast agents or EOB in nodules ≥ 1 cm in diameter. However, lesion should not show either marked T2 high SI or targetoid appearance on DWI or contrast-enhanced sequences. On CEUS as second-line examinations, major imaging features include arterial hyperenhancement and late (≥ 60 seconds) and mild washout, †In nodule(s) with some but not all aforementioned major imaging features of HCC, category of “probable” HCC can be assigned only when lesion fulfills at least one item from each of following two categories of ancillary imaging features. Two categories which make up ancillary imaging features are findings favoring malignancy in general (mild-to-moderate T2 hyperintensity, restricted diffusion, HBP hypointensity, interval growth) and those favoring HCC in particular (non-enhancing capsule, mosaic architecture, nodule-in-nodule appearance, fat or blood products in mass). These criteria should be applied only to lesion which shows neither marked T2 hyperintensity nor targetoid appearance on DWI or contrast-enhanced sequences. DWI = diffusion-weighted imaging, ECCM = extracellular contrast media, Gd-EOB-DTPA = gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid, HBP = hepatobiliary phase, KLCA-NCC = Korean Liver Cancer Association-National Cancer Center, LC = liver cirrhosis, MRI = magnetic resonance imaging, SI = signal intensity
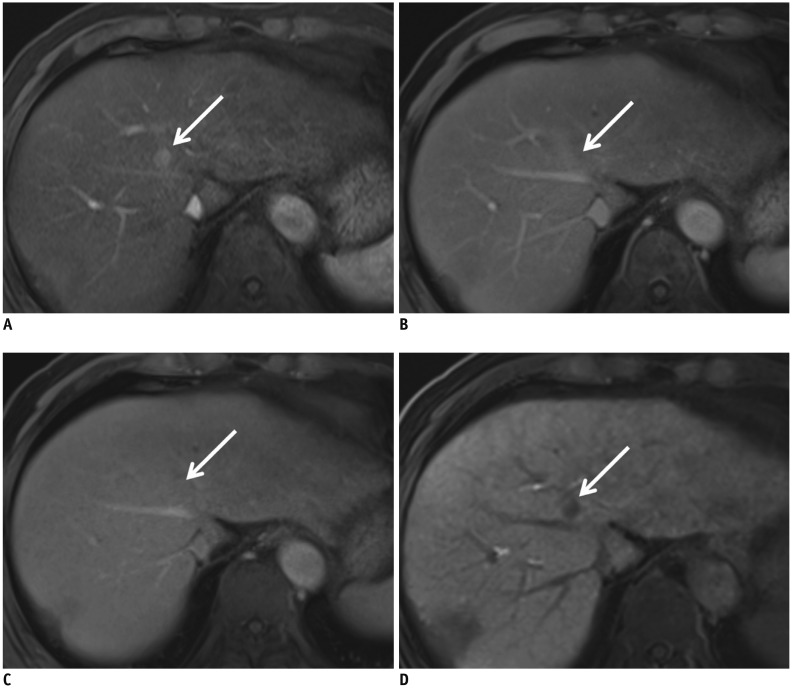
Fig. 4 Gadoxetic acid-enhanced MRI in 62-year-old man with CHB.On arterial phase MRI (A), 1.2-cm enhancing nodule is visualized in S4 (arrows) abutting middle hepatic vein. Nodule shows iso-, iso-, and hypointensity on portal (B); transitional (C); and hepatobiliary (D) phases, respectively. Lesion was pathologically confirmed as HCC. This nodule does not meet criteria of LR-5 according to Western guidelines; however, this nodule can be diagnosed as HCC according to updated 2018 KLCA-NCC guidelines.
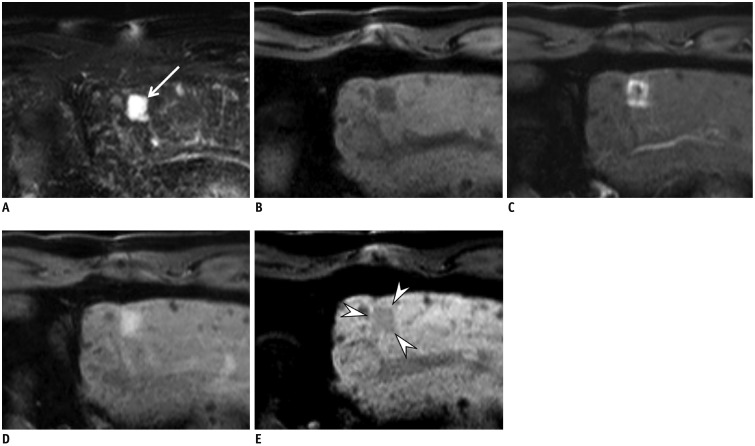
Fig. 5 Gadoxetic acid-enhanced MRI in 70-year-old man with CHB.On T2-weighted (A) and precontrast T1-weighted (B) MRI, 2-cm nodule (arrow) is seen with marked T2 hyperintensity and low T1 SI at subcapsular portion of segment 2 of liver. After contrast injection, lesion demonstrates nodular enhancement in arterial phase (C) and persistent enhancement in portal phase (D). Lesion (arrowheads) depicts hypointensity on HBP (E). Lesion was proved to be hemangioma by showing no interval change over years. Regardless of arterial enhancement with hepatobiliary defect, diagnosis of HCC cannot be made due to exclusion criteria of marked T2 hyperintensity according to updated KLCA-NCC guidelines version 2018.
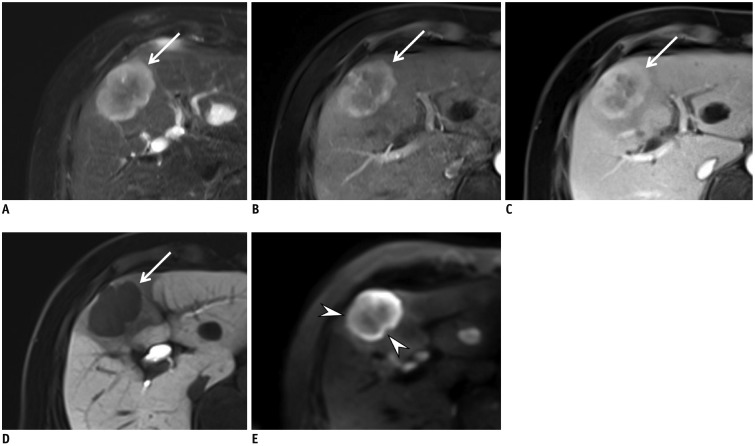
Fig. 6 Gadoxetic acid-enhanced MRI in 70-year-old woman with chronic hepatitis C.On fat-saturated T2-weighted image (A), approximately 5-cm mass (arrow) with mild hyperintensity is seen in segment 4 of liver. After gadoxetic acid injection, lesion (arrows) shows arterial hyperenhancement (B), isointensity on portal phase (C), and hypointensity on HBP (D). On diffusion-weighted image (E), mass (arrowheads) demonstrates peripheral hyperintensity with typical targetoid appearance. Mass was histopathologically confirmed as cholangiocarcinoma. Regardless of presence of arterial enhancement with hepatobiliary defect, diagnosis of HCC cannot be made due to exclusion criteria of targetoid appearance according to updated KLCA-NCC guidelines version 2018.
Reference
-
1. Choo SP, Tan WL, Goh BKP, Tai WM, Zhu AX. Comparison of hepatocellular carcinoma in Eastern versus Western populations. Cancer. 2016; 122:3430–3446. PMID: 27622302.
Article2. Altekruse SF, McGlynn KA, Reichman ME. Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol. 2009; 27:1485–1491. PMID: 19224838.
Article3. Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis. PLoS Med. 2014; 11:e1001624. PMID: 24691105.
Article4. Trevisani F, De Notariis S, Rapaccini G, Farinati F, Benvegnù L, Zoli M, et al. Semiannual and annual surveillance of cirrhotic patients for hepatocellular carcinoma: effects on cancer stage and patient survival (Italian experience). Am J Gastroenterol. 2002; 97:734–744. PMID: 11922571.
Article5. Ando E, Kuromatsu R, Tanaka M, Takada A, Fukushima N, Sumie S, et al. Surveillance program for early detection of hepatocellular carcinoma in Japan: results of specialized department of liver disease. J Clin Gastroenterol. 2006; 40:942–948. PMID: 17063116.6. Noda I, Kitamoto M, Nakahara H, Hayashi R, Okimoto T, Monzen Y, et al. Regular surveillance by imaging for early detection and better prognosis of hepatocellular carcinoma in patients infected with hepatitis C virus. J Gastroenterol. 2010; 45:105–112. PMID: 19866332.
Article7. Lopez PM, Villanueva A, Llovet JM. Systematic review: evidence-based management of hepatocellular carcinoma--an updated analysis of randomized controlled trials. Aliment Pharmacol Ther. 2006; 23:1535–1547. PMID: 16696801.8. Cruite I, Tang A, Sirlin CB. Imaging-based diagnostic systems for hepatocellular carcinoma. AJR Am J Roentgenol. 2013; 201:41–55. PMID: 23789657.
Article9. Tang A, Cruite I, Sirlin CB. Toward a standardized system for hepatocellular carcinoma diagnosis using computed tomography and MRI. Expert Rev Gastroenterol Hepatol. 2013; 7:269–279. PMID: 23445236.
Article10. Tang A, Cruite I, Mitchell DG, Sirlin CB. Hepatocellular carcinoma imaging systems: why they exist, how they have evolved, and how they differ. Abdom Radiol (NY). 2018; 43:3–12. PMID: 28840293.
Article11. Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018; 67:358–380. PMID: 28130846.
Article12. Yu JS, Kim KW, Kim EK, Lee JT, Yoo HS. Contrast enhancement of small hepatocellular carcinoma: usefulness of three successive early image acquisitions during multiphase dynamic MR imaging. AJR Am J Roentgenol. 1999; 173:597–604. PMID: 10470886.
Article13. Torzilli G, Minagawa M, Takayama T, Inoue K, Hui AM, Kubota K, et al. Accurate preoperative evaluation of liver mass lesions without fine-needle biopsy. Hepatology. 1999; 30:889–893. PMID: 10498639.
Article14. Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part I. Development, growth, and spread: key pathologic and imaging aspects. Radiology. 2014; 272:635–654. PMID: 25153274.
Article15. Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, et al. Diagnosis, staging and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology. 2018; 68:723–750. PMID: 29624699.
Article16. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018; 69:182–236. PMID: 29628281.17. Omata M, Cheng AL, Kokudo N, Kudo M, Lee JM, Jia J, et al. Asia-pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017; 11:317–370. PMID: 28620797.
Article18. CT/MRI LI-RADS®, version 2017. American College of Radiology Web site. Accessed April 3, 2019. https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2017.19. New: CT/MRI LI-RADS®, version 2018. American College of Radiology Web site. Accessed April 3, 2019. https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2018.20. Wald C, Russo MW, Heimbach JK, Hussain HK, Pomfret EA, Bruix J. New OPTN/UNOS policy for liver transplant allocation: standardization of liver imaging, diagnosis, classification, and reporting of hepatocellular carcinoma. Radiology. 2013; 266:376–382. PMID: 23362092.
Article21. Kudo M, Matsui O, Izumi N, Iijima H, Kadoya M, Imai Y, et al. JSH consensus-based clinical practice guidelines for the management of hepatocellular carcinoma: 2014 update by the liver cancer study group of Japan. Liver Cancer. 2014; 3:458–468. PMID: 26280007.
Article22. Korean Liver Cancer Study Group (KLCSG), National Cancer Center, Korea (NCC). 2014 Korean Liver Cancer Study Group-National Cancer Center Korea practice guideline for the management of hepatocellular carcinoma. Korean J Radiol. 2015; 16:465–522. PMID: 25995680.23. Gavriilidis P, Roberts KJ, Askari A, Sutcliffe RP, Huo TL, Liu PH, et al. Evaluation of the current guidelines for resection of hepatocellular carcinoma using the appraisal of guidelines for research and evaluation II instrument. J Hepatol. 2017; 67:991–998. PMID: 28690176.
Article24. Korean Liver Cancer Association and National Cancer Center (KLCA-NCC) Korea. 2018 Korean liver cancer association-national cancer center Korea practice guidelines for management of hepatocellular carcinoma. Gut Liver. 2019; 13:227–299. PMID: 31060120.25. Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part II. Extracellular agents, hepatobiliary agents, and ancillary imaging features. Radiology. 2014; 273:30–50. PMID: 25247563.
Article26. Kitao A, Matsui O, Yoneda N, Kozaka K, Shinmura R, Koda W, et al. The uptake transporter OATP8 expression decreases during multistep hepatocarcinogenesis: correlation with gadoxetic acid enhanced MR imaging. Eur Radiol. 2011; 21:2056–2066. PMID: 21626360.
Article27. Kogita S, Imai Y, Okada M, Kim T, Onishi H, Takamura M, et al. Gd-EOB-DTPA-enhanced magnetic resonance images of hepatocellular carcinoma: correlation with histological grading and portal blood flow. Eur Radiol. 2010; 20:2405–2413. PMID: 20490505.
Article28. Lee YJ, Lee JM, Lee JS, Lee HY, Park BH, Kim YH, et al. Hepatocellular carcinoma: diagnostic performance of multidetector CT and MR imaging-a systematic review and meta-analysis. Radiology. 2015; 275:97–109. PMID: 25559230.
Article29. Kim HD, Lim YS, Han S, An J, Kim GA, Kim SY, et al. Evaluation of early-stage hepatocellular carcinoma by magnetic resonance imaging with gadoxetic acid detects additional lesions and increases overall survival. Gastroenterology. 2015; 148:1371–1382. PMID: 25733098.
Article30. Joo I, Lee JM, Lee DH, Jeon JH, Han JK, Choi BI. Noninvasive diagnosis of hepatocellular carcinoma on gadoxetic acid-enhanced MRI: can hypointensity on the hepatobiliary phase be used as an alternative to washout? Eur Radiol. 2015; 25:2859–2868. PMID: 25773941.
Article31. Choi SH, Byun JH, Lim YS, Yu E, Lee SJ, Kim SY, et al. Diagnostic criteria for hepatocellular carcinoma 3 cm with hepatocyte-specific contrast-enhanced magnetic resonance imaging. J Hepatol. 2016; 64:1099–1107. PMID: 26820629.
Article32. Sangiovanni A, Manini MA, Iavarone M, Romeo R, Forzenigo LV, Fraquelli M, et al. The diagnostic and economic impact of contrast imaging techniques in the diagnosis of small hepatocellular carcinoma in cirrhosis. Gut. 2010; 59:638–644. PMID: 19951909.
Article33. Khalili K, Kim TK, Jang HJ, Haider MA, Khan L, Guindi M, et al. Optimization of imaging diagnosis of 1-2 cm hepatocellular carcinoma: an analysis of diagnostic performance and resource utilization. J Hepatol. 2011; 54:723–728. PMID: 21156219.34. Yoon JH, Park JW, Lee JM. Noninvasive diagnosis of hepatocellular carcinoma: elaboration on Korean Liver Cancer Study Group-National Cancer Center Korea practice guidelines compared with other guidelines and remaining issues. Korean J Radiol. 2016; 17:7–24. PMID: 26798212.
Article35. Korean Society of Abdominal Radiology. Diagnosis of hepatocellular carcinoma with gadoxetic acid-enhanced MRI: 2016 consensus recommendations of the Korean Society of Abdominal Radiology. Korean J Radiol. 2017; 18:427–443. PMID: 28458595.36. Song KD, Kim SH, Lim HK, Jung SH, Sohn I, Kim HS. Subcentimeter hypervascular nodule with typical imaging findings of hepatocellular carcinoma in patients with history of hepatocellular carcinoma: natural course on serial gadoxetic acid-enhanced MRI and diffusion-weighted imaging. Eur Radiol. 2015; 25:2789–2796. PMID: 25735515.
Article37. Yoon JH, Lee JM, Yang HK, Lee KB, Jang JJ, Han JK, et al. Non-hypervascular hypointense nodules ≥ 1 cm on the hepatobiliary phase of gadoxetic acid-enhanced magnetic resonance imaging in cirrhotic livers. Dig Dis. 2014; 32:678–689. PMID: 25376284.38. Choi JW, Lee JM, Kim SJ, Yoon JH, Baek JH, Han JK, et al. Hepatocellular carcinoma: imaging patterns on gadoxetic acid-enhanced MR images and their value as an imaging biomarker. Radiology. 2013; 267:776–786. PMID: 23401584.
Article39. Suh YJ, Kim MJ, Choi JY, Park YN, Park MS, Kim KW. Differentiation of hepatic hyperintense lesions seen on gadoxetic acid-enhanced hepatobiliary phase MRI. AJR Am J Roentgenol. 2011; 197:W44–W52. PMID: 21700994.
Article40. Davenport MS, Viglianti BL, Al-Hawary MM, Caoili EM, Kaza RK, Liu PS, et al. Comparison of acute transient dyspnea after intravenous administration of gadoxetate disodium and gadobenate dimeglumine: effect on arterial phase image quality. Radiology. 2013; 266:452–461. PMID: 23192781.
Article41. Pietryga JA, Burke LM, Marin D, Jaffe TA, Bashir MR. Respiratory motion artifact affecting hepatic arterial phase imaging with gadoxetate disodium: examination recovery with a multiple arterial phase acquisition. Radiology. 2014; 271:426–434. PMID: 24475864.
Article42. Bolondi L, Correas JM, Lencioni R, Weskott HP, Piscaglia F. New perspectives for the use of contrast-enhanced liver ultrasound in clinical practice. Dig Liver Dis. 2007; 39:187–195. PMID: 17208526.
Article43. Strobel D, Bernatik T, Blank W, Schuler A, Greis C, Dietrich CF, et al. Diagnostic accuracy of CEUS in the differential diagnosis of small (≤ 20 mm) and subcentimetric (≤ 10 mm) focal liver lesions in comparison with histology. Results of the DEGUM multicenter trial. Ultraschall Med. 2011; 32:593–597. PMID: 22161556.44. Kim TK, Noh SY, Wilson SR, Kono Y, Piscaglia F, Jang HJ, et al. Contrast-enhanced ultrasound (CEUS) liver imaging reporting and data system (LI-RADS) 2017 - a review of important differences compared to the CT/MRI system. Clin Mol Hepatol. 2017; 23:280–289. PMID: 28911220.
Article45. Kudo M. Defect reperfusion imaging with Sonazoid®: a breakthrough in hepatocellular carcinoma. Liver Cancer. 2016; 5:1–7. PMID: 26989655.
Article46. Maruyama H, Takahashi M, Ishibashi H, Yoshikawa M, Yokosuka O. Contrast-enhanced ultrasound for characterisation of hepatic lesions appearing non-hypervascular on CT in chronic liver diseases. Br J Radiol. 2012; 85:351–357. PMID: 21224305.
Article47. Takahashi M, Maruyama H, Shimada T, Kamezaki H, Sekimoto T, Kanai F, et al. Characterization of hepatic lesions (≤ 30 mm) with liver-specific contrast agents: a comparison between ultrasound and magnetic resonance imaging. Eur J Radiol. 2013; 82:75–84. PMID: 23116806.48. Wilson SR, Kim TK, Jang HJ, Burns PN. Enhancement patterns of focal liver masses: discordance between contrast-enhanced sonography and contrast-enhanced CT and MRI. AJR Am J Roentgenol. 2007; 189:W7–W12. PMID: 17579140.
Article49. Itai Y, Furui S, Ohtomo K, Kokubo T, Yamauchi T, Minami M, et al. Dynamic CT features of arterioportal shunts in hepatocellular carcinoma. AJR Am J Roentgenol. 1986; 146:723–727. PMID: 3006460.
Article50. Yu JS, Kim KW, Jeong MG, Lee JT, Yoo HS. Nontumorous hepatic arterial-portal venous shunts: MR imaging findings. Radiology. 2000; 217:750–756. PMID: 11110939.
Article51. Leoni S, Piscaglia F, Granito A, Borghi A, Galassi M, Marinelli S, et al. Characterization of primary and recurrent nodules in liver cirrhosis using contrast-enhanced ultrasound: which vascular criteria should be adopted? Ultraschall Med. 2013; 34:280–287. PMID: 23616066.
Article52. Claudon M, Dietrich CF, Choi BI, Cosgrove DO, Kudo M, Nolsøe CP, et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med. 2013; 34:11–29. PMID: 23129518.53. Bota S, Piscaglia F, Marinelli S, Pecorelli A, Terzi E, Bolondi L. Comparison of international guidelines for noninvasive diagnosis of hepatocellular carcinoma. Liver Cancer. 2012; 1:190–200. PMID: 24159584.
Article54. Italian Association for the Study of the Liver (AISF). AISF Expert Panel. AISF Coordinating Committee. Bolondi L, Cillo U, Colombo M, Craxi A, Farinati F, Giannini EG, et al. Position paper of the Italian association for the study of the liver (AISF): the multidisciplinary clinical approach to hepatocellular carcinoma. Dig Liver Dis. 2013; 45:712–723. PMID: 23769756.
Article55. Sherman M, Burak K, Maroun J, Metrakos P, Knox JJ, Myers RP, et al. Multidisciplinary Canadian consensus recommendations for the management and treatment of hepatocellular carcinoma. Curr Oncol. 2011; 18:228–240. PMID: 21980250.
Article56. Furlan A, Marin D, Cabassa P, Taibbi A, Brunelli E, Agnello F, et al. Enhancement pattern of small hepatocellular carcinoma (HCC) at contrast-enhanced us (CEUS), MDCT, and MRI: intermodality agreement and comparison of diagnostic sensitivity between 2005 and 2010 American Association for the Study of Liver Diseases (AASLD) guidelines. Eur J Radiol. 2012; 81:2099–2105. PMID: 21906896.
Article57. Forner A, Vilana R, Ayuso C, Bianchi L, Solé M, Ayuso JR, et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: prospective validation of the noninvasive diagnostic criteria for hepatocellular carcinoma. Hepatology. 2008; 47:97–104. PMID: 18069697.
Article58. Terzi E, Iavarone M, Pompili M, Veronese L, Cabibbo G, Fraquelli M, et al. Contrast ultrasound LI-RADS LR-5 identifies hepatocellular carcinoma in cirrhosis in a multicenter restropective study of 1,006 nodules. J Hepatol. 2018; 68:485–492. PMID: 29133247.
Article59. Galassi M, Iavarone M, Rossi S, Bota S, Vavassori S, Rosa L, et al. Patterns of appearance and risk of misdiagnosis of intrahepatic cholangiocarcinoma in cirrhosis at contrast enhanced ultrasound. Liver Int. 2013; 33:771–779. PMID: 23445369.
Article60. Vilana R, Forner A, Bianchi L, García-Criado A, Rimola J, de Lope CR, et al. Intrahepatic peripheral cholangiocarcinoma in cirrhosis patients may display a vascular pattern similar to hepatocellular carcinoma on contrast-enhanced ultrasound. Hepatology. 2010; 51:2020–2029. PMID: 20512990.
Article61. Li R, Zhang X, Ma KS, Li XW, Xia F, Zhong H, et al. Dynamic enhancing vascular pattern of intrahepatic peripheral cholangiocarcinoma on contrast-enhanced ultrasound: the influence of chronic hepatitis and cirrhosis. Abdom Imaging. 2013; 38:112–119. PMID: 22323003.
Article62. Chen LD, Xu HX, Xie XY, Xie XH, Xu ZF, Liu GJ, et al. Intrahepatic cholangiocarcinoma and hepatocellular carcinoma: differential diagnosis with contrast-enhanced ultrasound. Eur Radiol. 2010; 20:743–753. PMID: 19760416.
Article63. Wildner D, Bernatik T, Greis C, Seitz K, Neurath MF, Strobel D. CEUS in hepatocellular carcinoma and intrahepatic cholangiocellular carcinoma in 320 patients - early or late washout matters: a subanalysis of the DEGUM multicenter trial. Ultraschall Med. 2015; 36:132–139. PMID: 25812115.
Article64. Wildner D, Pfeifer L, Goertz RS, Bernatik T, Sturm J, Neurath MF, et al. Dynamic contrast-enhanced ultrasound (DCE-US) for the characterization of hepatocellular carcinoma and cholangiocellular carcinoma. Ultraschall Med. 2014; 35:522–527. PMID: 25202903.65. Piscaglia F, Kudo M, Han KH, Sirlin C. Diagnosis of hepatocellular carcinoma with non-invasive imaging: a plea for worldwide adoption of standard and precise terminology for describing enhancement criteria. Ultraschall Med. 2017; 38:9–11. PMID: 28249327.66. Piscaglia F, Wilson SR, Lyshchik A, Cosgrove D, Dietrich CF, Jang HJ, et al. American College of Radiology Contrast enhanced ultrasound Liver Imaging Reporting and Data System (CEUS LI-RADS) for the diagnosis of hepatocellular carcinoma: a pictorial essay. Ultraschall Med. 2017; 38:320–324. PMID: 28329875.67. Aubé C, Oberti F, Lonjon J, Pageaux G, Seror O, N’Kontchou G, et al. EASL and AASLD recommendations for the diagnosis of HCC to the test of daily practice. Liver Int. 2017; 37:1515–1525. PMID: 28346737.
Article68. American College of Radiology. Ultrasound LI-RADS® v2017. American College of Radiology Web site. Accessed January 1, 2019. https://www.acr.org/clinical-resources/reporting-and-data-systems/li-rads/ultrasound-li-rads-v2017.69. Joo I, Lee JM, Lee DH, Jeon JH, Han JK. Retrospective validation of a new diagnostic criterion for hepatocellular carcinoma on gadoxetic acid-enhanced MRI: can hypointensity on the hepatobiliary phase be used as an alternative to washout with the aid of ancillary features? Eur Radiol. 2019; 29:1724–1732. PMID: 30255250.
Article70. Farinati F, Sergio A, Baldan A, Giacomin A, Di Nolfo MA, Del Poggio P, et al. Early and very early hepatocellular carcinoma: when and how much do staging and choice of treatment really matter? A multi-center study. BMC Cancer. 2009; 9:33. PMID: 19171074.
Article71. Kim YY, An C, Kim S, Kim MJ. Diagnostic accuracy of prospective application of the liver imaging reporting and data system (LI-RADS) in gadoxetate-enhanced MRI. Eur Radiol. 2018; 28:2038–2046. PMID: 29230525.
Article72. Joo I, Lee JM, Lee DH, Ahn SJ, Lee ES, Han JK. Liver imaging reporting and data system v2014 categorization of hepatocellular carcinoma on gadoxetic acid-enhanced MRI: comparison with multiphasic multidetector computed tomography. J Magn Reson Imaging. 2017; 45:731–740. PMID: 27474328.
Article73. Choi SH, Lee SS, Kim SY, Park SH, Park SH, Kim KM, et al. Intrahepatic cholangiocarcinoma in patients with cirrhosis: differentiation from hepatocellular carcinoma by using gadoxetic acid-enhanced MR imaging and dynamic CT. Radiology. 2017; 282:771–781. PMID: 27797675.
Article74. Bolondi L. Screening for hepatocellular carcinoma in cirrhosis. J Hepatol. 2003; 39:1076–1084. PMID: 14642630.
Article75. Singal A, Volk ML, Waljee A, Salgia R, Higgins P, Rogers MA, et al. Meta-analysis: surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis. Aliment Pharmacol Ther. 2009; 30:37–47. PMID: 19392863.
Article76. Besa C, Lewis S, Pandharipande PV, Chhatwal J, Kamath A, Cooper N, et al. Hepatocellular carcinoma detection: diagnostic performance of a simulated abbreviated MRI protocol combining diffusion-weighted and T1-weighted imaging at the delayed phase post gadoxetic acid. Abdom Radiol (NY). 2017; 42:179–190. PMID: 27448609.
Article77. Marks RM, Ryan A, Heba ER, Tang A, Wolfson TJ, Gamst AC, et al. Diagnostic per-patient accuracy of an abbreviated hepatobiliary phase gadoxetic acid-enhanced MRI for hepatocellular carcinoma surveillance. AJR Am J Roentgenol. 2015; 204:527–535. PMID: 25714281.
Article78. Tanaka H, Iijima H, Nouso K, Aoki N, Iwai T, Takashima T, et al. Cost-effectiveness analysis on the surveillance for hepatocellular carcinoma in liver cirrhosis patients using contrast-enhanced ultrasonography. Hepatol Res. 2012; 42:376–384. PMID: 22221694.
Article79. Jang KM, Kim SH, Kim YK, Choi D. Imaging features of subcentimeter hypointense nodules on gadoxetic acid-enhanced hepatobiliary phase MR imaging that progress to hypervascular hepatocellular carcinoma in patients with chronic liver disease. Acta Radiol. 2015; 56:526–535. PMID: 24838304.
Article80. Wang JH, Changchien CS, Hu TH, Lee CM, Kee KM, Lin CY, et al. The efficacy of treatment schedules according to Barcelona clinic liver cancer staging for hepatocellular carcinoma-survival analysis of 3892 patients. Eur J Cancer. 2008; 44:1000–1006. PMID: 18337087.81. Hatanaka K, Kudo M, Minami Y, Maekawa K. Sonazoid-enhanced ultrasonography for diagnosis of hepatic malignancies: comparison with contrast-enhanced CT. Oncology. 2008; 75(Suppl 1):42–47.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imaging diagnosis of hepatocellular carcinoma: Future directions with special emphasis on hepatobiliary magnetic resonance imaging and contrast-enhanced ultrasound
- Comparison of international guidelines for noninvasive diagnosis of hepatocellular carcinoma: 2018 update
- Recent Updates of Abbreviated MRI for Hepatocellular Carcinoma Screening
- Sonazoid-enhanced ultrasonography for noninvasive imaging diagnosis of hepatocellular carcinoma: special emphasis on the 2022 KLCA-NCC guideline
- Diagnosis of Hepatocellular Carcinoma with Gadoxetic Acid-Enhanced MRI: 2016 Consensus Recommendations of the Korean Society of Abdominal Radiology
