Validation of the eighth edition of the American Joint Committee on Cancer staging system and proposal of an improved staging system for pancreatic ductal adenocarcinoma
- Affiliations
-
- 1Division of Hepato-Biliary and Pancreatic Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. drksc@amc.seoul.kr
- 2Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2439045
- DOI: http://doi.org/10.14701/ahbps.2019.23.1.46
Abstract
- BACKGROUNDS/AIMS
This study aimed to validate the eighth edition of the American Joint Committee on Cancer (AJCC) staging system for pancreatic adenocarcinoma and to propose an improved staging system for this disease.
METHODS
Between 2000 and 2014, 1656 patients underwent surgical resection for pancreatic ductal adenocarcinoma at Asan Medical Center, Seoul, South Korea. The 1169 patients included in this study were recategorized according to the eighth edition of the AJCC staging system. Patients were also categorized according to a new staging system, based on tumor size and number of metastatic lymph nodes.
RESULTS
The seventh edition of the AJCC staging system categorized 93.7% of patients as having stage T3 tumors. Stages were distributed more evenly with the eighth edition. In the N0 group, classification according to the seventh edition showed no statistically significant differences in survival rate between patients with T1 and T2 (p=0.717) and with IA and IB (p=0.717) tumors. Survival rates classified according to the eighth edition differed significantly for all pairs of T stages (p < 0.05). With both editions, N stages showed statistically significant differences (p < 0.05). Reanalysis showed that a staging system using a tumor size ≥3 cm and ≥1 metastatic lymph nodes was more predictive of survival rates.
CONCLUSIONS
Compared with the seventh edition, the eighth edition of the AJCC staging system for pancreatic adenocarcinoma showed a more even distribution in T stage but marginal differences in other stages. The proposed system, using tumor size and number of metastatic lymph nodes, was better at predicting survival.
Keyword
MeSH Terms
Figure
-
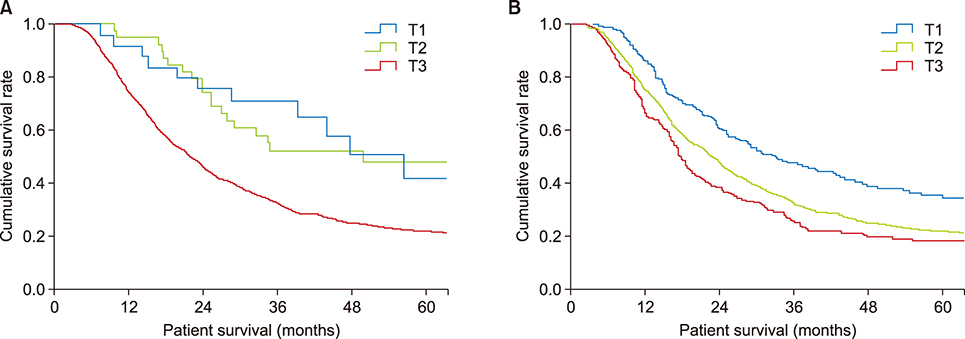
Fig. 1 Overall survival in N0 patients subcategorized by T stage (omitting those categorized as T4, M1, and R1 and those who received neoadjuvant chemotherapy). (A) Overall survival of patients classified by T stage according to the seventh AJCC staging system. Median survival was not assessed in the T1 group because the number of patients was too small. Median survival differed significantly in patients classified as T2 and T3 (64.6 vs. 30.46 months, p=0.026), but not in patients classified as T1 and T2 (p=0.717). (B) Overall survival of patients classified by T stage according to the eighth AJCC staging system. Median survival in patients classified as T1, T2, and T3 was 43.20, 32.32, and 23.46 months, respectively, with pairwise differences between T1 and T2 (p=0.045) and between T2 and T3 (p=0.049) being statistically significant.
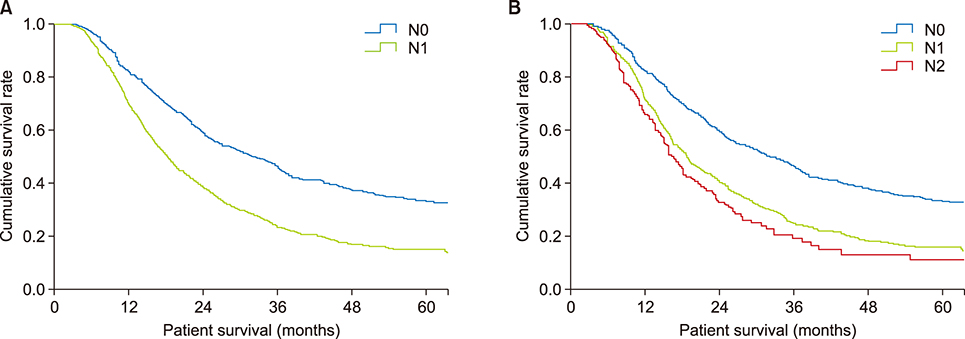
Fig. 2 Overall survival in patients subcategorized by N stage (omitting those with T4, M1, and R1 and those who received neoadjuvant chemotherapy). (A) Overall survival of patients classified by N stage according to the seventh AJCC staging system. Median survival differed significantly in patients classified as N0 and N1 (32.33 vs. 18.56 months, p<0.001). (B) Overall survival of patients classified by N stage according to the eighth AJCC staging system. Median overall survival in patients classified as N0, N1, and N2 was 32.33, 18.86, and 16.83 months, respectively, with pairwise differences between N0 and N1 (p<0.001) and between N1 and N2 (p=0.042) being statistically significant.

Fig. 3 Overall survival in patients subcategorized by stages (omitting those with R1 and those who received neoadjuvant chemotherapy). (A) Overall survival of patients classified by stage according to the seventh AJCC staging system. Median survival in patients with stage IA tumors was not determined because of the small number of patients. Median survival in patients classified as stages IB, IIA, IIB, III, and IV was 64.6, 29.9, 18.4, 13.2, and 13.1 months, respectively, with pairwise differences between patients with stages IB and IIA (p=0.026), IIA and IIB (p<0.001), and IIB and III (p=0.002) being statistically significant. (B) Overall survival of patients classified by stage according to the eighth AJCC staging system. Median survival in patients classified as stages IA, IB, IIA, IIB, III, and IV was 44.4, 31.5, 22.3, 18.9, 15.9, and 13.1 months, with pairwise differences between patients with stages IA and IB (p=0.045), IB and IIA (p=0.049), IIA and IIB (p=0.022), and IIB and III (p=0.010) being statistically significant.

Fig. 4 Overall survival in patients classified by suggested T and N stages (omitting those with T4, M1, and R1 tumors and those who received neoadjuvant chemotherapy). (A) Overall survival of suggested T stages based on tumor size <3 cm vs. ≥3 cm (p<0.001). (B) Overall survival at newly suggested N stages based on number of distant metastases 0 vs. ≥1 (p<0.001). (C) Overall survival of each group assorted by suggested T and N stages. Three groups were identified, consisting of patients with tumors staged as T1N0 (group 1), T2N0 and T1N1 (group 2), and T2N1 (group 3). Differences between patients classified as T1N0 and T2N0 (p<0.001) and those classified as T1N1 and T2N1 (p<0.001) were statistically significant, whereas those between patients classified as T2N0 and T1N1 (p=0.207) were not.
Reference
-
1. Conlon KC, Klimstra DS, Brennan MF. Long-term survival after curative resection for pancreatic ductal adenocarcinoma. Clinicopathologic analysis of 5-year survivors. Ann Surg. 1996; 223:273–279.2. Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am Coll Surg. 1999; 189:1–7.3. Kindler HL. Pancreatic cancer: an update. Curr Oncol Rep. 2007; 9:170–176.
Article4. Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg. 1993; 165:68–72. discussion 72-73.
Article5. Schnelldorfer T, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, et al. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg. 2008; 247:456–462.6. Nitecki SS, Sarr MG, Colby TV, van Heerden JA. Long-term survival after resection for ductal adenocarcinoma of the pancreas. Is it really improving? Ann Surg. 1995; 221:59–66.
Article7. Cleary SP, Gryfe R, Guindi M, Greig P, Smith L, Mackenzie R, et al. Prognostic factors in resected pancreatic adenocarcinoma: analysis of actual 5-year survivors. J Am Coll Surg. 2004; 198:722–731.8. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010; 17:1471–1474.
Article9. Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The eighth edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017; 67:93–99.
Article10. Varadhachary GR, Tamm EP, Abbruzzese JL, Xiong HQ, Crane CH, Wang H, et al. Borderline resectable pancreatic cancer: definitions, management, and role of preoperative therapy. Ann Surg Oncol. 2006; 13:1035–1046.
Article11. Bilimoria KY, Bentrem DJ, Ko CY, Tomlinson JS, Stewart AK, Winchester DP, et al. Multimodality therapy for pancreatic cancer in the U.S. : utilization, outcomes, and the effect of hospital volume. Cancer. 2007; 110:1227–1234.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Updated guidelines on the preoperative staging of thyroid cancer
- Assessment of the Prognostic Staging System of American Joint Committee on Cancer 8th Edition for Breast Cancer: Comparisons with the Conventional Anatomic Staging System
- A Comparison of Fifth-Edition and Sixth-Edition American Joint Committee Staging System for Sinonasal Squamous Cell Carcinoma
- Introduction of 7th AJCC TNM Staging for Hepatobiliary, Pancreatic Ampulla of Vater, Exocrine and Endocrine Cancers
- Introduction of 7th AJCC Cancer Staging: Gallbladder, Perihilar Bile Duct and Distal Common Bile Duct
