Acute Crit Care.
2018 Aug;33(3):162-169. 10.4266/acc.2018.00199.
Usefulness of Rotational Thromboelastometry as a Mortality Predictor of Hyperfibrinolysis in Patients with Severe Trauma
- Affiliations
-
- 1Department of Emergency Medicine, Pusan National University Hospital, Busan, Korea. jrmr9933@gmail.com
- 2Department of Trauma Surgery, Pusan National University Hospital, Busan, Korea.
- 3Department of Emergency Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea.
- KMID: 2436328
- DOI: http://doi.org/10.4266/acc.2018.00199
Abstract
- BACKGROUND
Hemorrhage is the major cause of traumatic death and the leading cause of preventable death. Hyperfibrinolysis is associated with trauma severity. Viscoelastic hemostatic assays show complete clot formation dynamics. The present study was designed to identify the relationship between hyperfibrinolysis and mortality, metabolic acidosis, and coagulopathy in patients with trauma.
METHODS
Patients with severe trauma (injury severity score [ISS] of 15 or higher) who were assessed using rotational thromboelastometry (ROTEM) were included in the present study from January 2017 to December 2017. Variables were obtained from the Korea Trauma Database or the medical charts of the patients. To identify whether hyperfibrinolysis is an independent predictor of mortality, univariate and multivariate Cox regression analyses were performed.
RESULTS
During the 1-year study period, 190 patients were enrolled. In total, 21 (11.1%) had hyperfibrinolysis according to the ROTEM analysis and 46 (24.2%) died. Patients with hyperfibrinolysis had a higher ISS (P=0.014) and mortality rate (P < 0.001) than did those without hyperfibrinolysis. In multivariate Cox analysis, hyperfibrinolysis (hazard ratio [HR], 4.960; 95% confidence interval [CI], 2.447 to 10.053), age (HR, 1.033; 95% CI, 1.013 to 1.055), lactic acid level (HR, 1.085; 95% CI, 1.003 to 1.173), and ISS (HR, 1.037; 95% CI, 1.004 to 1.071) were independent predictors of mortality.
CONCLUSIONS
Hyperfibrinolysis is associated with increased mortality, worse metabolic acidosis, and severe coagulopathy and is an independent predictor of mortality in patients with trauma.
Keyword
MeSH Terms
Figure
-
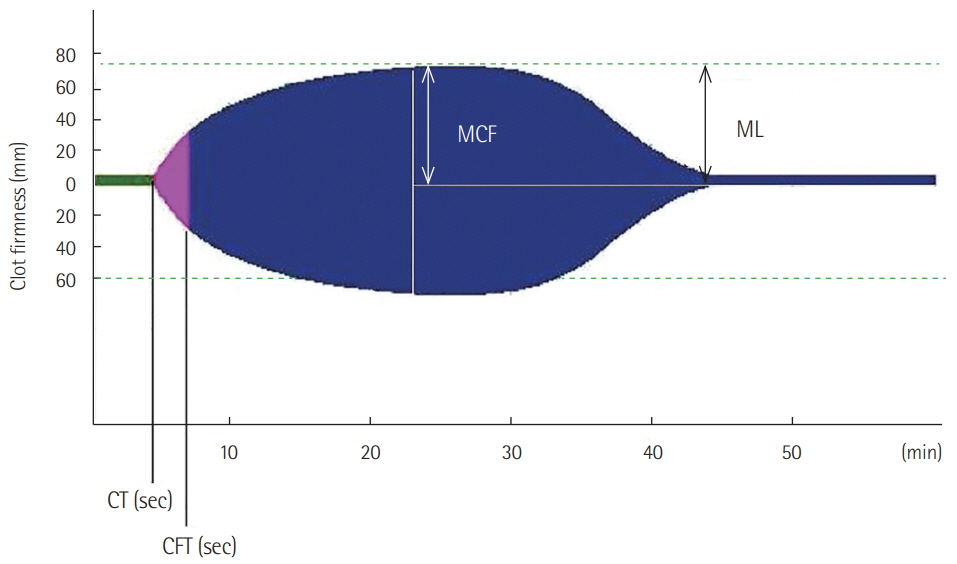
Figure 1. The parameters of rotational thromboelastometry. (1) Clotting time (CT): initiation of clotting; (2) clot formation time (CFT): time from clot initiation to a clot firmness of 20 mm; (3) maximum clot firmness (MCF): maximum clot strength; and (4) maximum lysis (ML): reduction of clot firmness after achieving MCF.

Figure 2. Hyperfibrinolysis in (A) INTEM, (B) EXTEM, and (C) FIBTEM. (D) The APTEM shows stable clot formation.
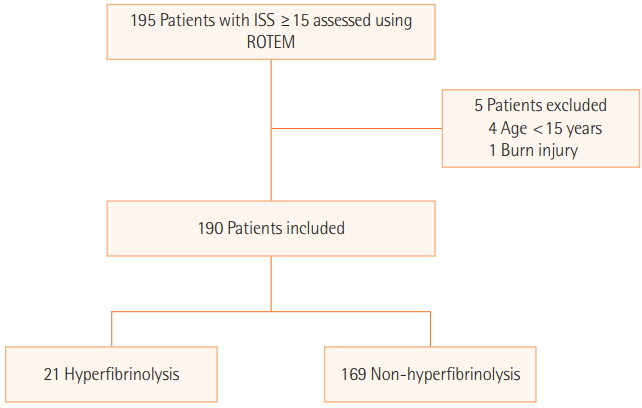
Figure 3. Patient flow. ISS: injury severity score; ROTEM: rotational thromboelastometry.
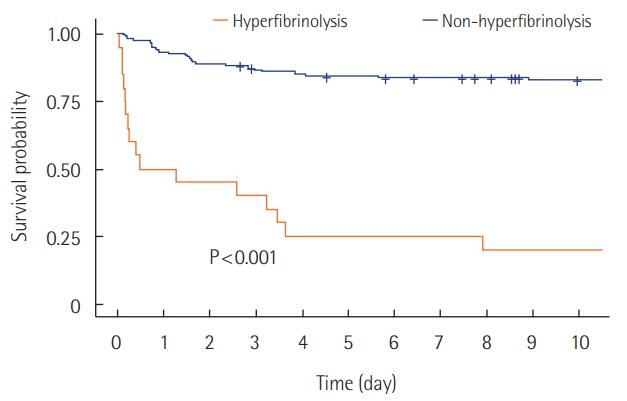
Figure 4. Kaplan-Meier survival curves showing mortality differences between patients with and without hyperfibrinolysis. P<0.001 by log-rank test.
Reference
-
1. Cothren CC, Moore EE, Hedegaard HB, Meng K. Epidemiology of urban trauma deaths: a comprehensive reassessment 10 years later. World J Surg. 2007; 31:1507–11.
Article2. Ramirez RJ, Spinella PC, Bochicchio GV. Tranexamic acid update in trauma. Crit Care Clin. 2017; 33:85–99.
Article3. Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003; 54:1127–30.
Article4. Davenport R. Pathogenesis of acute traumatic coagulopathy. Transfusion. 2013; 53 Suppl 1:23S–27S.
Article5. Cohen MJ, Call M, Nelson M, Calfee CS, Esmon CT, Brohi K, et al. Critical role of activated protein C in early coagulopathy and later organ failure, infection and death in trauma patients. Ann Surg. 2012; 255:379–85.
Article6. Gall LS, Brohi K, Davenport RA. Diagnosis and treatment of hyperfibrinolysis in trauma (a European Perspective). Semin Thromb Hemost. 2017; 43:224–34.
Article7. Theusinger OM, Wanner GA, Emmert MY, Billeter A, Eismon J, Seifert B, et al. Hyperfibrinolysis diagnosed by rotational thromboelastometry (ROTEM) is associated with higher mortality in patients with severe trauma. Anesth Analg. 2011; 113:1003–12.
Article8. Schöchl H, Frietsch T, Pavelka M, Jámbor C. Hyperfibrinolysis after major trauma: differential diagnosis of lysis patterns and prognostic value of thrombelastometry. J Trauma. 2009; 67:125–31.
Article9. Raza I, Davenport R, Rourke C, Platton S, Manson J, Spoors C, et al. The incidence and magnitude of fibrinolytic activation in trauma patients. J Thromb Haemost. 2013; 11:307–14.
Article10. Gall LS, Davenport RA. Fibrinolysis and antifibrinolytic treatment in the trauma patient. Curr Opin Anaesthesiol. 2018; 31:227–33.
Article11. Gonzalez E, Moore EE, Moore HB. Management of traumainduced coagulopathy with thrombelastography. Crit Care Clin. 2017; 33:119–34.
Article12. Liras IN, Cotton BA, Cardenas JC, Harting MT. Prevalence and impact of admission hyperfibrinolysis in severely injured pediatric trauma patients. Surgery. 2015; 158:812–8.
Article13. Moore HB, Moore EE, Gonzalez E, Chapman MP, Chin TL, Silliman CC, et al. Hyperfibrinolysis, physiologic fibrinolysis, and fibrinolysis shutdown: the spectrum of postinjury fibrinolysis and relevance to antifibrinolytic therapy. J Trauma Acute Care Surg. 2014; 77:811–7.14. Cardenas JC, Matijevic N, Baer LA, Holcomb JB, Cotton BA, Wade CE. Elevated tissue plasminogen activator and reduced plasminogen activator inhibitor promote hyperfibrinolysis in trauma patients. Shock. 2014; 41:514–21.
Article15. Carroll RC, Craft RM, Langdon RJ, Clanton CR, Snider CC, Wellons DD, et al. Early evaluation of acute traumatic coagulopathy by thrombelastography. Transl Res. 2009; 154:34–9.
Article16. Demetriades D, Martin M, Salim A, Rhee P, Brown C, Doucet J, et al. Relationship between American College of Surgeons trauma center designation and mortality in patients with severe trauma (injury severity score > 15). J Am Coll Surg. 2006; 202:212–5.17. Leemann H, Lustenberger T, Talving P, Kobayashi L, Bukur M, Brenni M, et al. The role of rotation thromboelastometry in early prediction of massive transfusion. J Trauma. 2010; 69:1403–8.
Article18. Lang T, Bauters A, Braun SL, Pötzsch B, von Pape KW, Kolde HJ, et al. Multi-centre investigation on reference ranges for ROTEM thromboelastometry. Blood Coagul Fibrinolysis. 2005; 16:301–10.
Article19. Levrat A, Gros A, Rugeri L, Inaba K, Floccard B, Negrier C, et al. Evaluation of rotation thrombelastography for the diagnosis of hyperfibrinolysis in trauma patients. Br J Anaesth. 2008; 100:792–7.
Article20. Kutcher ME, Cripps MW, McCreery RC, Crane IM, Greenberg MD, Cachola LM, et al. Criteria for empiric treatment of hyperfibrinolysis after trauma. J Trauma Acute Care Surg. 2012; 73:87–93.
Article21. Akay OM. The double hazard of bleeding and thrombosis in hemostasis from a clinical point of view: a global assessment by Rotational Thromboelastometry (ROTEM). Clin Appl Thromb Hemost. 2018; 24:850–8.
Article22. Gomez-Builes JC, Acuna SA, Nascimento B, Madotto F, Rizoli SB. Harmful or physiologic: diagnosing fibrinolysis shutdown in a trauma cohort with rotational thromboelastometry. Anesth Analg. 2018; Apr. 19. [Epub]. https://doi.org/10.1213/ANE.0000000000003341.
Article23. Ives C, Inaba K, Branco BC, Okoye O, Schochl H, Talving P, et al. Hyperfibrinolysis elicited via thromboelastography predicts mortality in trauma. J Am Coll Surg. 2012; 215:496–502.
Article24. Hunt H, Stanworth S, Curry N, Woolley T, Cooper C, Ukoumunne O, et al. Thromboelastography (TEG) and rotational thromboelastometry (ROTEM) for trauma induced coagulopathy in adult trauma patients with bleeding. Cochrane Database Syst Rev. 2015; (2):CD010438.
Article25. Rugeri L, Levrat A, David JS, Delecroix E, Floccard B, Gros A, et al. Diagnosis of early coagulation abnormalities in trauma patients by rotation thrombelastography. J Thromb Haemost. 2007; 5:289–95.
Article26. Kashuk JL, Moore EE, Wohlauer M, Johnson JL, Pezold M, Lawrence J, et al. Initial experiences with point-of-care rapid thrombelastography for management of life-threatening postinjury coagulopathy. Transfusion. 2012; 52:23–33.
Article27. Gonzalez E, Moore EE, Moore HB, Chapman MP, Chin TL, Ghasabyan A, et al. Goal-directed hemostatic resuscitation of trauma-induced coagulopathy: a pragmatic randomized clinical trial comparing a viscoelastic assay to conventional coagulation assays. Ann Surg. 2016; 263:1051–9.28. Veigas PV, Callum J, Rizoli S, Nascimento B, da Luz LT. A systematic review on the rotational thrombelastometry (ROTEM®) values for the diagnosis of coagulopathy, prediction and guidance of blood transfusion and prediction of mortality in trauma patients. Scand J Trauma Resusc Emerg Med. 2016; 24:114.
Article29. Prat NJ, Meyer AD, Ingalls NK, Trichereau J, DuBose JJ, Cap AP. Rotational thromboelastometry significantly optimizes transfusion practices for damage control resuscitation in combat casualties. J Trauma Acute Care Surg. 2017; 83:373–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rotational thromboelastometry for diagnosing sudden hyperfibrinolysis immediately after cardiopulmonary bypass during cardiac surgery
- The role of rotational thromboelastometry during the COVID-19 pandemic: a narrative review
- Prediction of Mid-term Platelet Transfusion in Stable Trauma Patients Using Rotational Thromboelastometry
- Influence of alcohol consumption on blood coagulation in rotational thromboelastometry (ROTEM): an in-vivo study
- The prognostic usefulness of the lactate/albumin ratio for predicting multiple organ dysfunction syndrome in severe trauma
