Acute Ischemic Stroke in Moyamoya Syndrome Associated with Thyrotoxicosis
- Affiliations
-
- 1Department of Neurology, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. brainyrk@gmail.com
- 2Department of Neurology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- KMID: 2434840
- DOI: http://doi.org/10.18700/jnc.180046
Abstract
- BACKGROUND
A few cases of moyamoya syndrome associated with thyrotoxicosis have been reported. However, studies on the association of hyperthyroidism with moyamoya syndrome are insufficient.
CASE REPORT
Here we report a case of hyperthyroidism associated with moyamoya syndrome in a 41-year-old woman with aphasia and right side weakness. Brain imaging revealed acute cerebral infarction of left middle cerebral artery territory and occlusion of bilateral distal internal carotid arteries.
CONCLUSION
Antithyroid medication stabilized the patient's neurologic deterioration, suggesting that thyrotoxicosis could aggravate acute cerebral infarction caused by moyamoya syndrome.
MeSH Terms
Figure
-
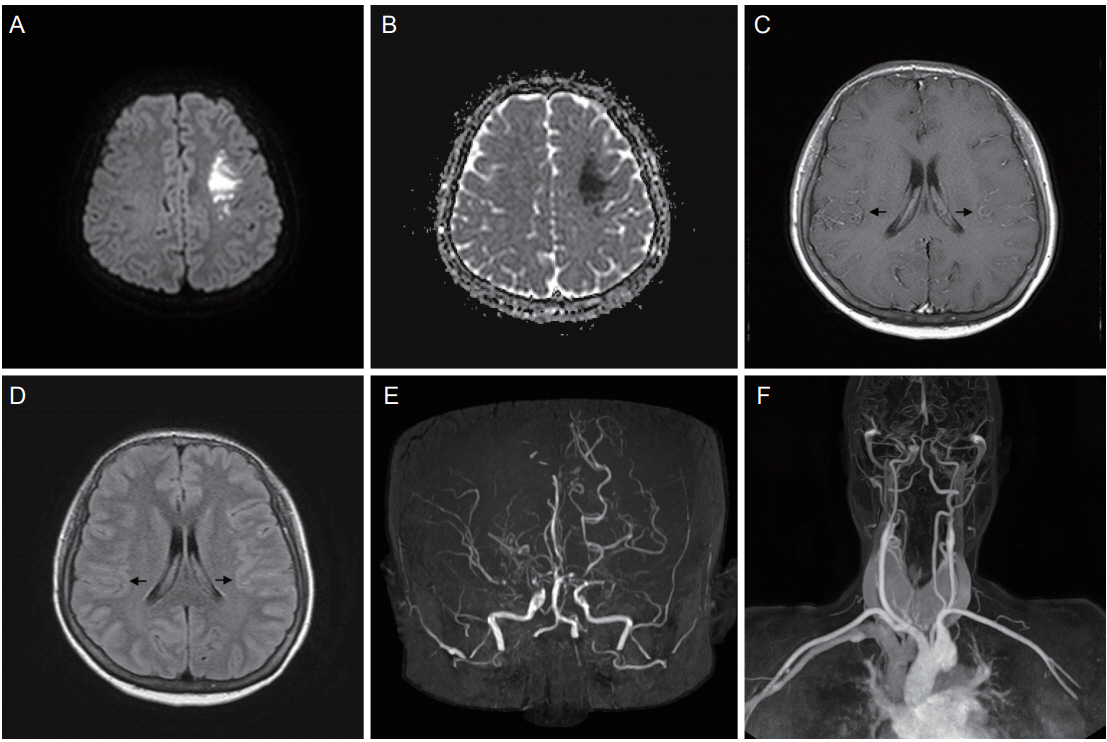
Figure 1. Brain DWI, ADC, T1WI with gadolinium enhancement, FLAIR images, and head and neck MR angiographic images (A-F). DWI shows acute cerebral infarction on left middle cerebral artery territory (A) with low signal on ADC (B). T1WI images with gadolinium enhancement reveals prominent leptomeningeal enhancement in bilateral hemispheres (black arrows, C). FLAIR images show high signal intensity in the same area (black arrows, D). MR angiographic imaging reveals total occlusion of bilateral distal internal carotid arteries (E, F). DWI, diffusion-weight imaging; ADC, apparent diffusion coefficient; T1WI, T1-weighted images; FLAIR, fluidattenuated inversion recovery; MR, magnetic resonance.
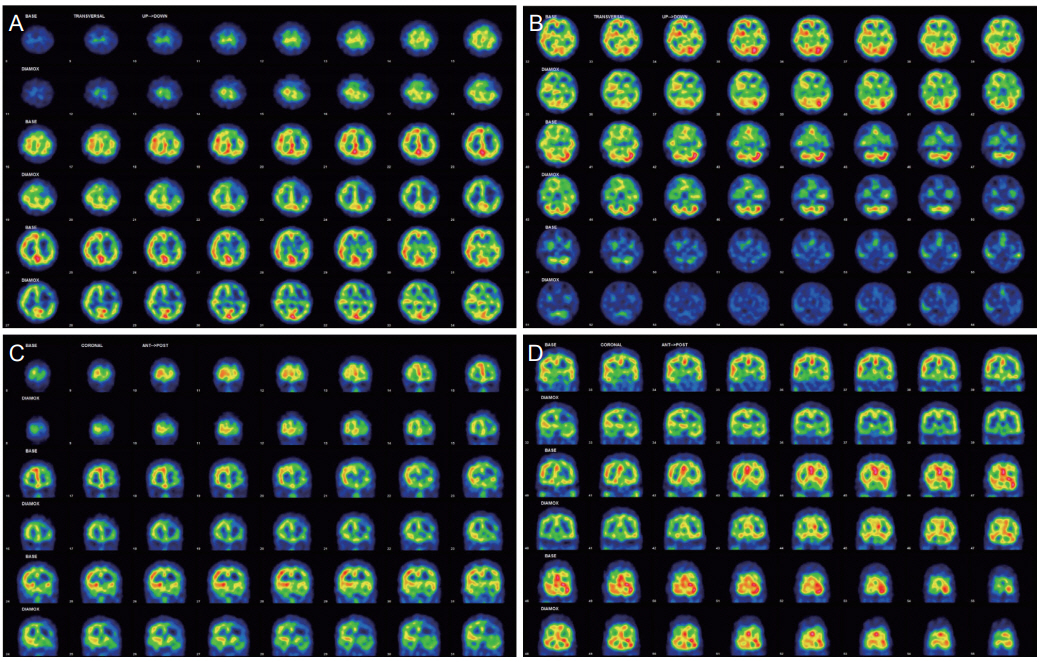
Figure 2. Brain single photon emission computed tomography (A-D). Odd lines show basal imaging and even lines show post-zoladin imaging. These imaging confirmed decreased perfusion and collateral blood reservoir lacking in left frontotemporal lobe and right temporal lobe.
Cited by 1 articles
-
Acute cerebral infarction combined with a thyroid storm in a patient with both Moyamoya syndrome and Graves’ disease
Jong Han Gill, Taek Kyun Nam, Hoon Kyo Jung, Kyung Min Jang, Hyun Ho Choi, Yong Sook Park, Jeong Taik Kwon
J Cerebrovasc Endovasc Neurosurg. 2022;24(2):160-165. doi: 10.7461/jcen.2021.E2021.07.003.
Reference
-
1. Scott RM, Smith ER. Moyamoya disease and moyamoya syndrome. N Engl J Med. 2009; 360:1226–37.
Article2. Kim JS. Moyamoya disease: epidemiology, clinical features, and diagnosis. J Stroke. 2016; 18:2–11.
Article3. Lee JY, Kim SK. Update of moyamoya disease. J Korean Med Assoc. 2007; 50:1109–18.
Article4. Seo KD, Suh SH, Kim YB, Kim JH, Ahn SJ, Kim DS, et al. Ivy sign on fluid-attenuated inversion recovery images in moyamoya disease: correlation with clinical severity and old brain lesions. Yonsei Med J. 2015; 56:1322–7.
Article5. Polikar R, Burger AG, Scherrer U, Nicod P. The thyroid and the heart. Circulation. 1993; 87:1435–41.
Article6. Napoli R, Biondi B, Guardasole V, Matarazzo M, Pardo F, Angelini V, et al. Impact of hyperthyroidism and its correction on vascular reactivity in humans. Circulation. 2001; 104:3076–80.
Article7. Ohba S, Nakagawa T, Murakami H. Concurrent Graves’ disease and intracranial arterial stenosis/occlusion: special considerations regarding the state of thyroid function, etiology, and treatment. Neurosurg Rev. 2011; 34:297–304. discussion 304.
Article8. Tendler BE, Shoukri K, Malchoff C, MacGillivray D, Duckrow R, Talmadge T, et al. Concurrence of Graves’ disease and dysplastic cerebral blood vessels of the moyamoya variety. Thyroid. 1997; 7:625–9.
Article9. Kim SJ, Heo KG, Shin HY, Bang OY, Kim GM, Chung CS, et al. Association of thyroid autoantibodies with moyamoyatype cerebrovascular disease: a prospective study. Stroke. 2010; 41:173–6.10. Jung CH, Rhee EJ, Shin HS, Jo SK, Won JC, Park CY, et al. Higher serum free thyroxine levels are associated with coronary artery disease. Endocr J. 2008; 55:819–26.
Article11. Choi YH, Chung JH, Bae SW, Lee WH, Jeong EM, Kang MG, et al. Severe coronary artery spasm can be associated with hyperthyroidism. Coron Artery Dis. 2005; 16:135–9.
Article12. Al Jaber J, Haque S, Noor H, Ibrahim B, Al Suwaidi J. Thyrotoxicosis and coronary artery spasm: case report and review of the literature. Angiology. 2010; 61:807–12.
Article13. Lee SY, Rhee CM, Leung AM, Braverman LE, Brent GA, Pearce EN. A review: radiographic iodinated contrast media-induced thyroid dysfunction. J Clin Endocrinol Metab. 2015; 100:376–83.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Ischemic Stroke in Moyamoya Disease Associated With Thyrotoxic Crisis
- Allergic Reaction Induced Brainstem Stroke in a Patient With Moyamoya Disease: A Case Report
- A Case of Moyamoya Disease in a Girl with Thyrotoxicosis
- Fatal ischemic stroke in a case of progressive moyamoya vasculopathy associated with uncontrolled thyrotoxicosis
- Concurrence of Diabetic Ketoacidosis and Acute Ischemic Stroke due to Moyamoya Disease
