Ann Clin Neurophysiol.
2019 Jan;21(1):66-69. 10.14253/acn.2019.21.1.66.
Orthostatic hypotension with meningoencephalitis involving the rostral ventrolateral medulla
- Affiliations
-
- 1Department of Neurology, Bundang Jesaeng General Hospital, Seongnam, Korea.
- 2Department of Neurology, Sanggye Paik Hospital, Inje University College of Medcine, Seoul, Korea. jykimmd@paik.ac.kr
- KMID: 2434191
- DOI: http://doi.org/10.14253/acn.2019.21.1.66
Abstract
- Orthostatic hypotension (OH) is commonly associated with autonomic failure in the peripheral nervous system. Less often it is related to central lesions in brainstem and cerebellum. We describe a patient with OH associated with tuberculosis meningoencephalitis involving the brainstem including rostral ventrolateral medulla. This is the first case of OH resulting from focal lesions in the dorsal medulla in a patient with meningoencephalitis.
MeSH Terms
Figure
-
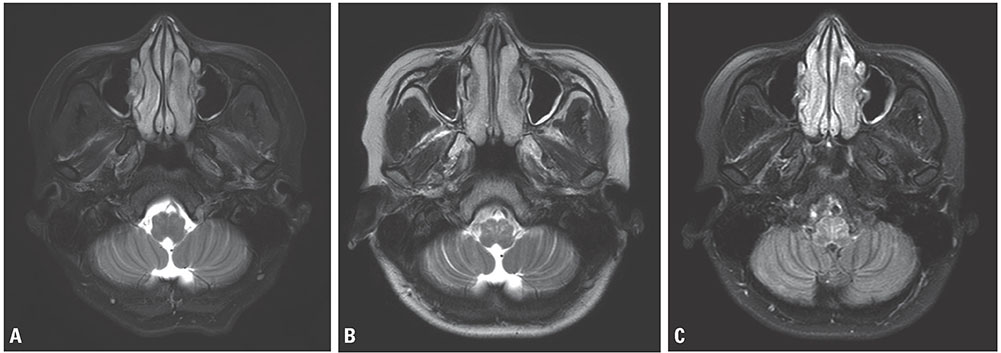
Fig. 1 (A) Axial T2-weighted magnetic resonance imaging showing leptomeningeal enhancement without parenchymal changes. (B, C) Axial T2 and flair showing aggravated involvement of the medullary lesion, including the rostal ventrolateral medulla (RVLM) in follow-up magnetic resonance imaging.
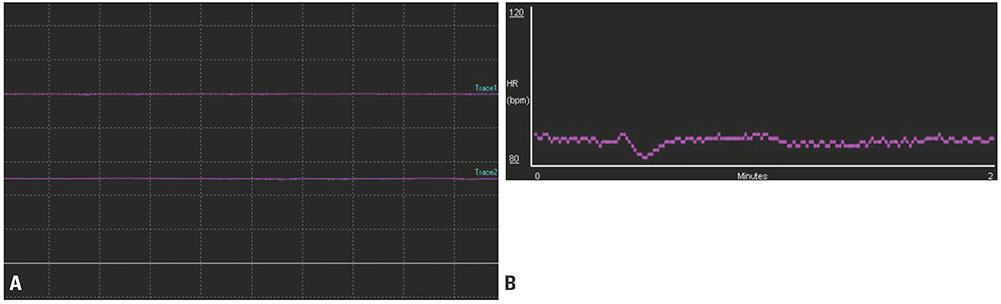
Fig. 2 Autonomic function test showed the sympathetic failure. (A) Absence of sympathetic skin response. (B) Valsalva maneuver test showed a transient decrease during first few seconds by activation of baroreceptors, but not followed by compensatory tachycardia.
Reference
-
1. Freeman R, Wieling W, Axelrod FB, Benditt DG, Benarroch E, Biaggioni I, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011; 21:69–72.
Article2. Low PA, Tomalia VA. Orthostatic hypotension: mechanisms, causes, management. J Clin Neurol. 2015; 11:220–226.
Article3. Telerman-Toppet N, Vanderhaeghen JJ, Warszawski M. Orthostatic hypotension with lower brain stem glioma. J Neurol Neurosurg Psychiatry. 1982; 45:1147–1150.
Article4. Derrey S, Maltête D, Ahtoy P, Fregey P, Proust F. Severe orthostatic hypotension and intramedullary tumor: a case report and review of the literature. Neurochirurgie. 2009; 55:589–594.5. Hocker S, Hoover JM, Puffer RC, Meyer FB. Orthostatic hypotension following resection of a dorsal medullary hemangioblastoma. Neurocrit Care. 2012; 16:306–310.
Article6. Idiaquez J, Araya P, Benarroch E. Orthostatic hypotension associated with dorsal medullary cavernous angioma. Acta Neurol Scand. 2009; 119:45–48.
Article7. Ikumi K, Ando T, Asahina M. A case of neuromyelitis optica spectrum disorder presenting with severe orthostatic hypotension. Rinsho Shinkeigaku. 2015; 55:759–762.
Article8. Kim HA, Lee H. Orthostatic hypotension in acute cerebellar infarction. J Neurol. 2016; 263:120–126.
Article9. Dormer KJ, Anwar M, Ashlock SR, Ruggiero DA. Organization of presumptive catecholamine-synthesizing neurons in the canine medulla oblongata. Brain Res. 1993; 601:41–64.
Article10. Arango V, Ruggiero DA, Callaway JL, Anwar M, Mann JJ, Reis DJ. Catecholaminergic neurons in the ventrolateral medulla and nucleus of the solitary tract in the human. J Comp Neurol. 1988; 273:224–240.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Orthostatic Dizziness Developed by Brainstem Tumor
- Orthostatic Intolerance Syndrome
- The Role of the Vestibular System in Modulating Blood Pressure of Sinoaortic Denervated Rats
- Analysis of the Baroreceptor and Vestibular Receptor Inputs in the Rostral Ventrolateral Medulla following Hypotension in Conscious Rats
- Role of Vestibulosympathetic Reflex on Orthostatic Hypotension in Rats
