Mycobacterium avium Complex Infection-Related Immune Reconstitution Inflammatory Syndrome Mimicking Lymphoma in an Human Immunodeficiency Virus-Infected Patient
- Affiliations
-
- 1Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University Medical College, Seoul, Korea.
- 2Division of Infectious Diseases, Department of Internal Medicine, Gil Medical Center, Gachon University College of Medicine, Incheon, Korea. helppl@gachon.ac.kr
- KMID: 2429939
- DOI: http://doi.org/10.3947/ic.2018.50.4.350
Abstract
- In acquired immunodeficiency syndrome (AIDS) patients, immune reconstitution inflammatory syndrome (IRIS) due to Mycobacterium avium complex (MAC) infection is one of the most difficult IRIS types to manage. We report an unusual case of MAC-associated IRIS. At first the patient was diagnosed human immunodeficiency virus (HIV) infection after he was admitted with pneumocystis pneumonia. After starting antiretroviral therapy he presented unmasked IRIS with MAC infection. Next, he was hospitalized with continuous loose stools and new-onset fever. Investigation included computed tomography (CT), which showed homogeneous enhancement and enlargement of the lymph nodes (LN), elevation of ferritin (>1,650 ng/mL) and lactate dehydrogenase (306 IU/L) levels, and F- fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) scan, which showed increased FDG uptake. These findings were highly indicative of lymphoma. We performed laparoscopic biopsy of the mesenteric LN, and the biopsy culture grew MAC. So we made a diagnosis of MAC-associated. Therefore, IRIS must be considered as a possible diagnosis when AIDS patients develop new symptoms or exhibit exacerbations of existing symptoms. Furthermore the biopsies should be conducted.
MeSH Terms
Figure
-
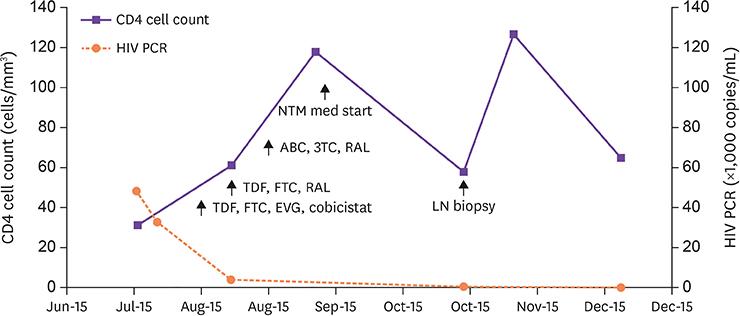
Figure 1 The series of CD4 cell count and HIV RNA PCR level. The arrows indicate the date of important medication or procedure were conducted. HIV, human immunodeficiency virus; RNA, ribonucleic acid; PCR, polymerase chain reaction; NTM, non-tuberculous mycobacterium; ABC, abacavir; 3TC, lamivudine; RAL, raltegravir; TDF, tenofovir disproxil; FTC, emtricitabine; LN, lymph node; EVG, elvitegravir.
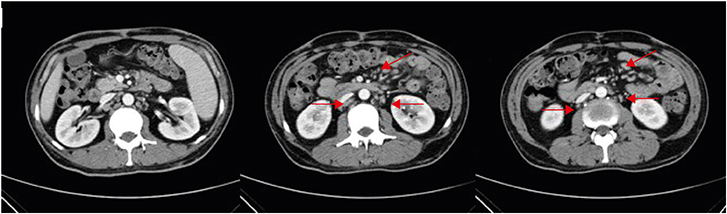
Figure 2 Abdomen/pelvic computed tomography axial plane shows multiple borderline size lymph nodes, paraaortic, aortocaval, retrocaval, and mesentery (red arrows).(Sixteen days after starting HAART). HAART, highly active antiretroviral therapy.
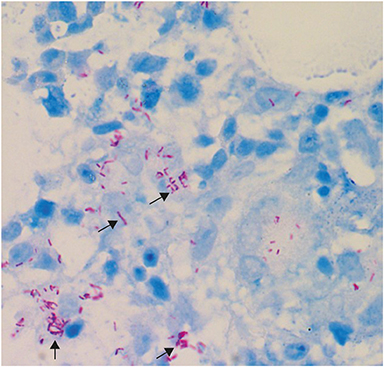
Figure 3 Bone marrow biopsy specimen revealed positive staining for acid fast bacilli.ositive (black arrows). (Ziehl-Neelsen stain, x 400).
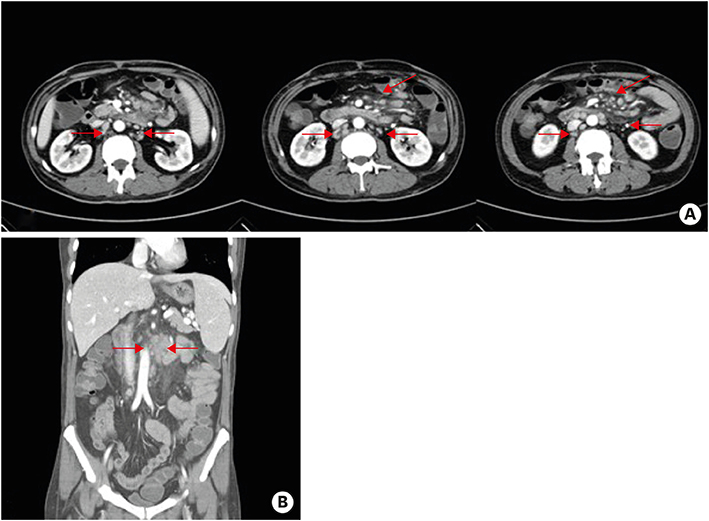
Figure 4 (A) Abdomen/pelvic computed tomography axial plane shows multiple lymph nodes enlargement along mesentery (red arrows, Thirty four days of starting anti-MAC chemotherapy); (B) Abdomen/pelvic computed tomography shows multiple lymph nodes enlargement along mesentery (red arrows). MAC, Mycobacterium avium complex.
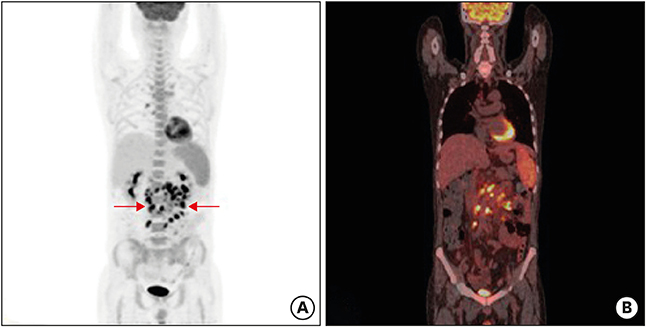
Figure 5 (A) Positron emission tomography image shows multiple enlarged hypermetabolic LNs in mesentery and retroperitoneum of abdomen, right retrocrural area (maximum standard uptake value = 13.4), right lower paratracheal, subcarinal and right hilar area and diffuse hypermetabolic activity in spleen and bone marrow (red arrows); (B) positron emission tomography/computed tomography image.
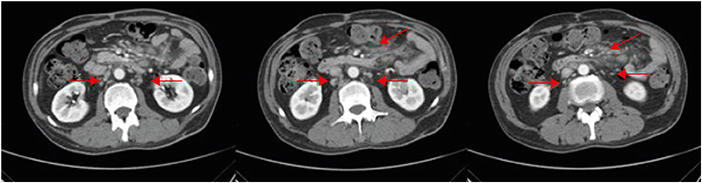
Figure 6 After 10 months of first visit, follow up abdomen/pelvic computed tomography shows slightly decreased size, but still remained multiple enlarged lymph nodes along mesentery (red arrows).
Reference
-
1. Chaisson RE, Moore RD, Richman DD, Keruly J, Creagh T. Incidence and natural history of Mycobacterium avium-complex infections in patients with advanced human immunodeficiency virus disease treated with zidovudine. The Zidovudine Epidemiology Study Group. Am Rev Respir Dis. 1992; 146:285–289.
Article2. Karakousis PC, Moore RD, Chaisson RE. Mycobacterium avium complex in patients with HIV infection in the era of highly active antiretroviral therapy. Lancet Infect Dis. 2004; 4:557–565.
Article3. Phillips P, Bonner S, Gataric N, Bai T, Wilcox P, Hogg R, O'Shaughnessy M, Montaner J. Nontuberculous mycobacterial immune reconstitution syndrome in HIV-infected patients: spectrum of disease and long-term follow-up. Clin Infect Dis. 2005; 41:1483–1497.
Article4. Powles T, Matthews G, Bower M. AIDS related systemic non-Hodgkin's lymphoma. Sex Transm Infect. 2000; 76:335–341.
Article5. Huhn GD, Badri S, Vibhakar S, Tverdek F, Crank C, Lubelchek R, Max B, Simon D, Sha B, Adeyemi O, Herrera P, Tenorio A, Kessler H, Barker D. Early development of non-hodgkin lymphoma following initiation of newer class antiretroviral therapy among HIV-infected patients - implications for immune reconstitution. AIDS Res Ther. 2010; 7:44.
Article6. Lapadula G, Soria A, Bandera A, Squillace N, Sabbatini F, Franzetti F, Migliori GB, Gori A. Unmasking tuberculosis in the era of antiretroviral treatment. Eur Respir J. 2012; 39:1064–1075.
Article7. Girardi E, Sabin CA, d'Arminio Monforte A, Hogg B, Phillips AN, Gill MJ, Dabis F, Reiss P, Kirk O, Bernasconi E, Grabar S, Justice A, Staszewski S, Fätkenheuer G, Sterne JA; Antiretroviral Therapy Cohort Collaboration. Incidence of tuberculosis among HIV-infected patients receiving highly active antiretroviral therapy in Europe and North America. Clin Infect Dis. 2005; 41:1772–1782.
Article8. Ko J, Shin B, Lee SS, Lim KS, Lee WJ, Yoo JR, Kang CI. Immune reconstitution inflammatory syndrome presenting as cutaneous miliary tuberculosis in an HIV-infected patient. Korean J Med. 2014; 86:647–650.
Article9. Murdoch DM, Venter WD, Van Rie A, Feldman C. Immune reconstitution inflammatory syndrome (IRIS): review of common infectious manifestations and treatment options. AIDS Res Ther. 2007; 4:9.
Article10. Wu UI, Chen MY, Hu RH, Hsieh SM, Sheng WH, Lo YC, Hung CC, Chang SC. Peritonitis due to Mycobacterium avium complex in patients with AIDS: report of five cases and review of the literature. Int J Infect Dis. 2009; 13:285–290.
Article11. Müller M, Wandel S, Colebunders R, Attia S, Furrer H, Egger M. IeDEA Southern and Central Africa. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta-analysis. Lancet Infect Dis. 2010; 10:251–261.
Article12. Sathekge M, Maes A, Kgomo M, Van de Wiele C. Fluorodeoxyglucose uptake by lymph nodes of HIV patients is inversely related to CD4 cell count. Nucl Med Commun. 2010; 31:137–140.
Article13. Yang ZG, Min PQ, Sone S, He ZY, Liao ZY, Zhou XP, Yang GQ, Silverman PM. Tuberculosis versus lymphomas in the abdominal lymph nodes: evaluation with contrast-enhanced CT. AJR Am J Roentgenol. 1999; 172:619–623.
Article14. Remick SC. Acquired immunodeficiency syndrome-related Non-Hodgkin lymphoma. Cancer Contr. 1995; 2:97–103.15. Barrington SF, O'Doherty MJ. Limitations of PET for imaging lymphoma. Eur J Nucl Med Mol Imaging. 2003; 30:Suppl 1. S117–S127.
Article16. Ngeow JY, Quek RH, Ng DC, Hee SW, Tao M, Lim LC, Tan YH, Lim ST. High SUV uptake on FDG-PET/CT predicts for an aggressive B-cell lymphoma in a prospective study of primary FDG-PET/CT staging in lymphoma. Ann Oncol. 2009; 20:1543–1547.
Article17. Del Giudice G, Bianco A, Cennamo A, Santoro G, Bifulco M, Marzo C, Mazzarella G. Lung and nodal involvement in nontuberculous mycobacterial disease: PET/CT role. Biomed Res Int. 2015; 2015:353202.
Article18. Namkoong H, Fujiwara H, Ishii M, Yagi K, Haraguchi M, Matsusaka M, Suzuki S, Asakura T, Asami T, Saito F, Fukunaga K, Tasaka S, Betsuyaku T, Hasegawa N. Immune reconstitution inflammatory syndrome due to Mycobacterium avium complex successfully followed up using 18 F-fluorodeoxyglucose positron emission tomography-computed tomography in a patient with human immunodeficiency virus infection: a case report. BMC Med Imaging. 2015; 15:24.
Article19. Sathekge M, Maes A, Van de Wiele C. FDG-PET imaging in HIV infection and tuberculosis. Semin Nucl Med. 2013; 43:349–366.
Article20. Schöder H, Gönen M. Screening for cancer with PET and PET/CT: potential and limitations. J Nucl Med. 2007; 48:Suppl 1. 4S–18S.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Herpes Zoster Immune Reconstitution Inflammatory Syndrome in a HIV-infected Patient: Case Report and Literature Review
- Immune Reconstitution Inflammatory Syndrome Presenting as Cutaneous Miliary Tuberculosis in an HIV-Infected Patient
- Simultaneous Diagnosis of Pneumococcal Sepsis and Disseminated Mycobacterium avium Complex Infection in a Patient with Acquired Immunodeficiency Syndrome
- Paradoxical Cryptococcal Meningitis Immune Reconstitution Inflammatory Syndrome in a Patient with Human Immunodeficiency Virus Infection: Matching Clinical Findings with MRI Findings
- A Case of Mesenteric Lymphadenitis Due to Mycobacterium avium Complex Infection in the Acquired Immunodeficiency Syndrome Patient
