Ann Rehabil Med.
2018 Oct;42(5):682-689. 10.5535/arm.2018.42.5.682.
Influence of Hip Fracture on Knee Pain During Postoperative Rehabilitation
- Affiliations
-
- 1Department of Rehabilitation Medicine, Dankook University College of Medicine, Cheonan, Korea. magnarbor@dankook.ac.kr
- 2Department of Nanobiomedical Science & WCU Research Center, Dankook University, Cheonan, Korea.
- 3Institute of Tissue Regeneration Engineering, Dankook University, Cheonan, Korea.
- KMID: 2429197
- DOI: http://doi.org/10.5535/arm.2018.42.5.682
Abstract
OBJECTIVE
To investigate whether fracture type, surgical procedure, or fracture grade affect knee pain during postoperative rehabilitation after a hip fracture.
METHODS
We conducted a retrospective case-controlled study of 139 patients during postoperative rehabilitation after surgery for hip fractures. Patients were divided into two groups: patients experiencing knee pain during the first week of postoperative rehabilitation, and patients without knee pain. We compared the types of fracture, surgical procedure, and fracture grade between the two groups.
RESULTS
We enrolled 52 patients (37.4%) with knee pain during the first weeks of postoperative rehabilitation. For type of fracture, knee pain was more common with intertrochanteric fracture than with femur neck fracture (48.8% vs. 21.1%, respectively; p=0.001). For the surgical procedure, there was no significant difference between the groups. For the fracture grade, the grades classified as unstable fractures were more common in the group of intertrochanteric fracture patients with knee pain than in those without knee pain (74.1% vs. 36.4%, respectively; p=0.002).
CONCLUSION
Intertrochanteric fracture affected knee pain after hip fracture surgery more than did femur neck fracture, particularly in unstable fractures. Furthermore, there was no difference in each fracture type according to the surgical procedure. Careful examination and management for knee pain is needed in patients with hip fracture surgery.
Keyword
MeSH Terms
Figure
-
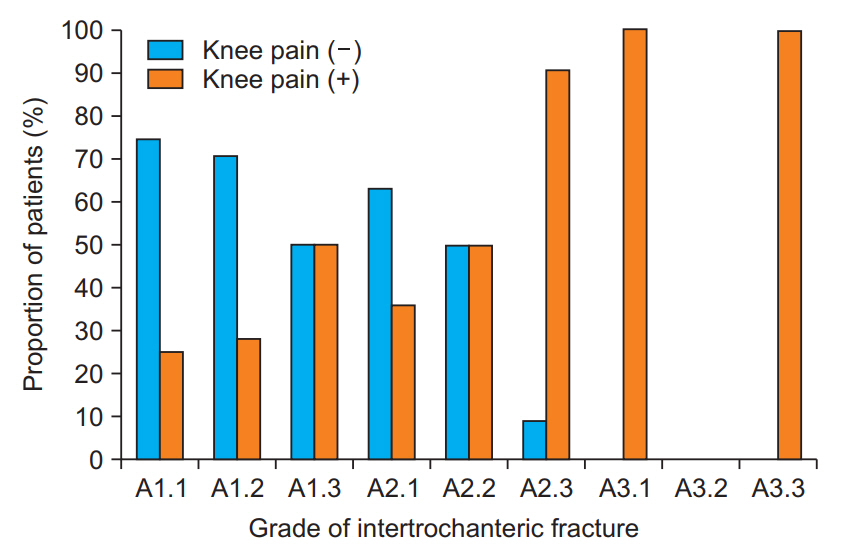
Fig. 1. Proportion of patients with and without knee pain according to grade of intertrochanteric fracture. AO/OTA alphanumeric classification was used to classify intertrochanteric fractures. The proportion of patients with knee pain increases in proportion to the grade. AO/OTA, Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association.
Reference
-
1. Lee SR, Ha YC, Kang H, Park YG, Nam KW, Kim SR. Morbidity and mortality in Jeju residents over 50-years of age with hip fracture with mean 6-year follow-up: a prospective cohort study. J Korean Med Sci. 2013; 28:1089–94.
Article2. Yoon HK, Park C, Jang S, Jang S, Lee YK, Ha YC. Incidence and mortality following hip fracture in Korea. J Korean Med Sci. 2011; 26:1087–92.
Article3. Choi HJ, Shin CS, Ha YC, Jang S, Jang S, Park C, et al. Burden of osteoporosis in adults in Korea: a national health insurance database study. J Bone Miner Metab. 2012; 30:54–8.
Article4. Ha YC, Kim TY, Lee A, Lee YK, Kim HY, Kim JH, et al. Current trends and future projections of hip fracture in South Korea using nationwide claims data. Osteoporos Int. 2016; 27:2603–9.
Article5. Muraki S, Akune T, Oka H, En-Yo Y, Yoshida M, Nakamura K, et al. Prevalence of falls and the association with knee osteoarthritis and lumbar spondylosis as well as knee and lower back pain in Japanese men and women. Arthritis Care Res (Hoboken). 2011; 63:1425–31.
Article6. Muraki S, Akune T, Oka H, Ishimoto Y, Nagata K, Yoshida M, et al. Physical performance, bone and joint diseases, and incidence of falls in Japanese men and women: a longitudinal cohort study. Osteoporos Int. 2013; 24:459–66.
Article7. Harris I, Hatfield A, Donald G, Walton J. Outcome after intramedullary nailing of femoral shaft fractures. ANZ J Surg. 2003; 73:387–9.
Article8. Wolinsky PR, McCarty E, Shyr Y, Johnson K. Reamed intramedullary nailing of the femur: 551 cases. J Trauma. 1999; 46:392–9.9. Braten M, Terjesen T, Rossvoll I. Femoral shaft fractures treated by intramedullary nailing: a follow-up study focusing on problems related to the method. Injury. 1995; 26:379–83.
Article10. Ostrum RF, Agarwal A, Lakatos R, Poka A. Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma. 2000; 14:496–501.11. Ricci WM, Bellabarba C, Evanoff B, Herscovici D, Di-Pasquale T, Sanders R. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma. 2001; 15:161–9.
Article12. Toms AD, Morgan-Jones RL, Spencer-Jones R. Intramedullary femoral nailing: removing the nail improves subjective outcome. Injury. 2002; 33:247–9.
Article13. Tornetta P 3rd, Tiburzi D. Antegrade or retrograde reamed femoral nailing: a prospective, randomised trial. J Bone Joint Surg Br. 2000; 82:652–4.14. Christodoulou AG, Givissis P, Antonarakos PD, Petsatodis GE, Hatzokos I, Pournaras JD. Knee joint effusion following ipsilateral hip surgery. J Orthop Surg (Hong Kong). 2010; 18:309–11.
Article15. Harato K, Yoshida H. Pseudogout at the knee joint will frequently occur after hip fracture and lead to the knee pain in the early postoperative period. J Orthop Surg Res. 2015; 10:4.
Article16. Pun WK, Chow SP, Chan KC, Ip FK, Leong JC. Effusions in the knee in elderly patients who were operated on for fracture of the hip. J Bone Joint Surg Am. 1988; 70:117–8.
Article17. Shahid MS, Murphy D, O’Donnell T, Ryan E, Kaliszer MM, Masterson E. A prospective study for evaluation of knee effusion after hip surgery. Ir Med J. 2002; 95:140–1.18. Jensen JS. Classification of trochanteric fractures. Acta Orthop Scand. 1980; 51:803–10.
Article19. Andersen E, Jorgensen LG, Hededam LT. Evans’ classification of trochanteric fractures: an assessment of the interobserver and intraobserver reliability. Injury. 1990; 21:377–8.
Article20. Gehrchen PM, Nielsen JO, Olesen B. Poor reproducibility of Evans’ classification of the trochanteric fracture: assessment of 4 observers in 52 cases. Acta Orthop Scand. 1993; 64:71–2.
Article21. Ahn H, Court-Brown CM, McQueen MM, Schemitsch EH. The use of hospital registries in orthopaedic surgery. J Bone Joint Surg Am. 2009; 91 Suppl 3:68–72.
Article22. Meling T, Harboe K, Enoksen CH, Aarflot M, Arthursson AJ, Soreide K. How reliable and accurate is the AO/OTA comprehensive classification for adult long-bone fractures? J Trauma Acute Care Surg. 2012; 73:224–31.
Article23. Sonawane DV. Classifications of intertrochanteric fractures and their clinical importance. Trauma Int. 2015; 1:7–11.24. Frandsen PA, Andersen E, Madsen F, Skjodt T. Garden’s classification of femoral neck fractures: an assessment of inter-observer variation. J Bone Joint Surg Br. 1988; 70:588–90.
Article25. Mears SC. Classification and surgical approaches to hip fractures for nonsurgeons. Clin Geriatr Med. 2014; 30:229–41.
Article26. Guss DA. Hip fracture presenting as isolated knee pain. Ann Emerg Med. 1997; 29:418–20.
Article27. Mitani S, Shimizu M, Abo M, Hagino H, Kurozawa Y. Risk factors for second hip fractures among elderly patients. J Orthop Sci. 2010; 15:192–7.
Article28. Omsland TK, Emaus N, Tell GS, Ahmed LA, Center JR, Nguyen ND, et al. Ten-year risk of second hip fracture: a NOREPOS study. Bone. 2013; 52:493–7.
Article29. Yamanashi A, Yamazaki K, Kanamori M, Mochizuki K, Okamoto S, Koide Y, et al. Assessment of risk factors for second hip fractures in Japanese elderly. Osteoporos Int. 2005; 16:1239–46.
Article30. Muraki S, Akune T, Ishimoto Y, Nagata K, Yoshida M, Tanaka S, et al. Risk factors for falls in a longitudinal population-based cohort study of Japanese men and women: the ROAD Study. Bone. 2013; 52:516–23.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postoperative Rehabilitation after Hip Fracture: A Literature Review
- Repeated Periprosthethic Femoral Fracture in a Below Knee Amputee with Ipsilateral Cementless Total Hip Arthroplasty: A Case Report
- Combined Ipsilateral Fracture and Dislocation of Hip, Knee and Foot Joints: A Case Report
- Total Hip Arthroplasty for Ankylosed Hip
- Fracture of the Medial Tibial Condyle in Unicompartmental Knee Arthroplasty: Report of 3 Cases
