J Korean Med Assoc.
2018 Oct;61(10):616-622. 10.5124/jkma.2018.61.10.616.
Causes, diagnosis, and treatment of pediatric osteoporosis
- Affiliations
-
- 1Department of Pediatrics, Korea Cancer Center Hospital, Seoul, Korea. limjs@kcch.re.kr
- KMID: 2426485
- DOI: http://doi.org/10.5124/jkma.2018.61.10.616
Abstract
- Osteoporosis was once thought to be a disease of the elderly. Now, there is universal agreement that osteoporosis has a pediatric origin. If individuals fail to achieve optimal peak bone mass and strength in childhood and adolescence, the development of osteoporosis later in life becomes more likely. Furthermore, increased knowledge and improved care for children with genetic disease and chronic illnesses has led to many children living long enough to develop osteoporosis and fractures even in childhood or adolescence. Thus, early interventions including nutrition, exercise, and pharmacological treatment are paramount. The objective of this review is to help clinicians diagnose and manage children at a high risk of osteoporosis. This article also reviews the latest advances in the treatment of pediatric osteoporosis including Korean experiences.
Keyword
MeSH Terms
Figure
-
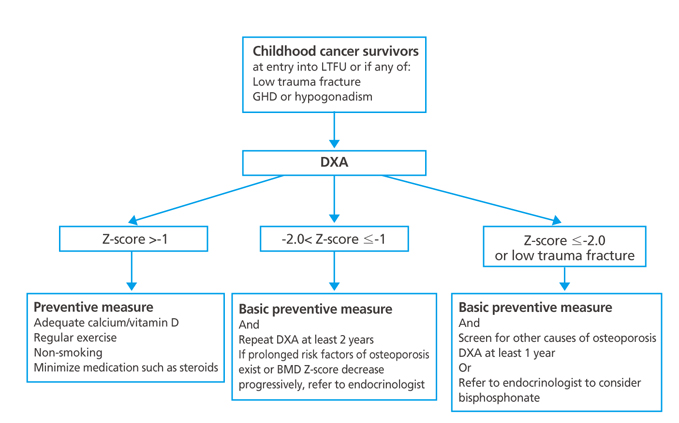
Figure 1 Algorithm to prevent osteoporosis in childhood cancer survivors. LTFU, long-term follow-up; GHD, growth hormone deficiency; DXA, dual energy X-ray absorptiometry; BMD, bone mineral density. Reproduced from Kang MJ, et al. Korean J Pediatr 2013;56:60-67, according to the Creative Commons license [20].
Reference
-
1. Riggs BL, Melton LJ. Osteoporosis: etiology, diagnosis, and management. New York: Raven Press;1988.2. Ma NS, Gordon CM. Pediatric osteoporosis: where are we now? J Pediatr. 2012; 161:983–990.
Article3. Heaney RP, Abrams S, Dawson-Hughes B, Looker A, Marcus R, Matkovic V, Weaver C. Peak bone mass. Osteoporos Int. 2000; 11:985–1009.
Article4. Lim JS. Pediatric dual-energy X-ray absorptiometry: interpretation and clinical and research application. Korean J Pediatr. 2010; 53:286–293.
Article5. Saraff V, Hogler W. Endocrinology and adolescence: Osteoporosis in children: diagnosis and management. Eur J Endocrinol. 2015; 173:R185–R197.
Article6. Osteoporosis prevention, diagnosis, and therapy. NIH Consens Statement. 2000; 17:1–45.7. Bishop N, Arundel P, Clark E, Dimitri P, Farr J, Jones G, Makitie O, Munns CF, Shaw N. International Society of Clinical Densitometry. Fracture prediction and the definition of osteoporosis in children and adolescents: the ISCD 2013 Pediatric Official Positions. J Clin Densitom. 2014; 17:275–280.
Article8. Lim JS, Hwang JS, Lee JA, Kim DH, Park KD, Cheon GJ, Shin CH, Yang SW. Bone mineral density according to age, bone age, and pubertal stages in Korean children and adolescents. J Clin Densitom. 2010; 13:68–76.
Article9. Yi KH, Hwang JS, Kim EY, Lee JA, Kim DH, Lim JS. Reference values for bone mineral density according to age with body size adjustment in Korean children and adolescents. J Bone Miner Metab. 2014; 32:281–289.
Article10. Goulding A, Jones IE, Taylor RW, Manning PJ, Williams SM. More broken bones: a 4-year double cohort study of young girls with and without distal forearm fractures. J Bone Miner Res. 2000; 15:2011–2018.
Article11. Venturi G, Tedeschi E, Mottes M, Valli M, Camilot M, Viglio S, Antoniazzi F, Tato L. Osteogenesis imperfecta: clinical, biochemical and molecular findings. Clin Genet. 2006; 70:131–139.
Article12. Lim JS. Treatments of osteoporosis in pediatric fields. J Korean Soc Pediatr Endocrinol. 2006; 11:138–147.13. Krassas GE. Idiopathic juvenile osteoporosis. Ann N Y Acad Sci. 2000; 900:409–412.
Article14. Lim JS, Lee DH. Changes in bone mineral density and body composition of children with well-controlled homocystinuria caused by CBS deficiency. Osteoporos Int. 2013; 24:2535–2538.
Article15. Ward LM, Glorieux FH. The spectrum of pediatric osteoporosis. In : Glorieux FH, Pettifor JM, Juppner H, editors. Pediatric bone: biology and disease. Boston: Academic Press;2003. p. 401–441.16. Jung KJ, Kwon SS, Chung CY, Lee KM, Sung KH, Cho BC, Chung MK, Moon SJ, Kim J, Park MS. Association of gross motor function classification system level and school attendance with bone mineral density in patients with cerebral palsy. J Clin Densitom. 2016; 10. 11. [Epub]. https://doi.org/10.1016/j.jocd.2016.09.002.
Article17. Laakso S, Valta H, Verkasalo M, Toiviainen-Salo S, Makitie O. Compromised peak bone mass in patients with inflammatory bowel disease: a prospective study. J Pediatr. 2014; 164:1436–1443.18. Kyriakou A, Shepherd S, Mason A, Ahmed SF. Prevalence of vertebral fractures in children with suspected osteoporosis. J Pediatr. 2016; 179:219–225.
Article19. Soyka LA, Grinspoon S, Levitsky LL, Herzog DB, Klibanski A. The effects of anorexia nervosa on bone metabolism in female adolescents. J Clin Endocrinol Metab. 1999; 84:4489–4496.
Article20. Kang MJ, Lim JS. Bone mineral density deficits in childhood cancer survivors: Pathophysiology, prevalence, screening, and management. Korean J Pediatr. 2013; 56:60–67.
Article21. Choi YJ, Park SY, Cho WK, Lee JW, Cho KS, Park SH, Hahn SH, Jung MH, Chung NG, Cho B, Suh BK, Kim HK. Factors related to decreased bone mineral density in childhood cancer survivors. J Korean Med Sci. 2013; 28:1632–1638.
Article22. Kang MJ, Kim SM, Lee YA, Shin CH, Yang SW, Lim JS. Risk factors for osteoporosis in long-term survivors of intracranial germ cell tumors. Osteoporos Int. 2012; 23:1921–1929.
Article23. Atkinson SA, Halton JM, Bradley C, Wu B, Barr RD. Bone and mineral abnormalities in childhood acute lymphoblastic leukemia: influence of disease, drugs and nutrition. Int J Cancer Suppl. 1998; 11:35–39.
Article24. Fratzl-Zelman N, Valta H, Pereira RC, Misof BM, Roschger P, Jalanko H, Wesseling-Perry K, Klaushofer K, Makitie O. Abnormally high and heterogeneous bone matrix mineralization after childhood solid organ transplantation: a complex pathology of low bone turnover and local defects in mineralization. J Bone Miner Res. 2017; 32:1116–1125.
Article25. Children's Oncology Group. Long-term follow-up guidelines for survivors of childhood, adolescent, and young adult cancers, ver. 4.0 [Internet]. Philadelphia: Children's Oncology Group;c2018. cited 2018 Jun 15. Available from: http://survivorshipguidelines.org/.26. Lee WT, Leung SS, Wang SH, Xu YC, Zeng WP, Lau J, Oppenheimer SJ, Cheng JC. Double-blind, controlled calcium supplementation and bone mineral accretion in children accustomed to a low-calcium diet. Am J Clin Nutr. 1994; 60:744–750.27. Greene DA, Naughton GA. Calcium and vitamin-D supplementation on bone structural properties in peripubertal female identical twins: a randomised controlled trial. Osteoporos Int. 2011; 22:489–498.
Article28. Ross AC, Taylor CL, Yaktine AL, Del Valle HB. Dietary reference intakes for calcium and vitamin D. Washington, DC: The National Academies Press;2011.29. Kim SH, Oh MK, Namgung R, Park MJ. Prevalence of 25-hydroxyvitamin D deficiency in Korean adolescents: association with age, season and parental vitamin D status. Public Health Nutr. 2014; 17:122–130.
Article30. Bass SL, Saxon L, Daly RM, Turner CH, Robling AG, Seeman E, Stuckey S. The effect of mechanical loading on the size and shape of bone in pre-, peri-, and postpubertal girls: a study in tennis players. J Bone Miner Res. 2002; 17:2274–2280.
Article31. Russell RG. Bisphosphonates: mode of action and pharmacology. Pediatrics. 2007; 119:Suppl 2. S150–S162.
Article32. Glorieux FH, Bishop NJ, Plotkin H, Chabot G, Lanoue G, Travers R. Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med. 1998; 339:947–952.
Article33. Choi JH, Shin YL, Yoo HW. Short-term efficacy of monthly pamidronate infusion in patients with osteogenesis imperfecta. J Korean Med Sci. 2007; 22:209–212.
Article34. Lee J, Yoon J, Lee YA, Lim JS, Shin CH, Yang SW. Pamidronate therapy in children and adolescents with secondary osteoporosis. J Korean Soc Pediatr Endocrinol. 2011; 16:178–184.
Article35. Moon SJ, An YM, Kim SK, Kwon YS, Lee JE. The effect of low-dose intravenous bisphosphonate treatment on osteoporosis in children with quadriplegic cerebral palsy. Korean J Pediatr. 2017; 60:403–407.
Article36. Kim SD, Cho BS. Pamidronate therapy for preventing steroid-induced osteoporosis in children with nephropathy. Nephron Clin Pract. 2006; 102:c81–c87.
Article37. Ward L, Tricco AC, Phuong P, Cranney A, Barrowman N, Gaboury I, Rauch F, Tugwell P, Moher D. Bisphosphonate therapy for children and adolescents with secondary osteoporosis. Cochrane Database Syst Rev. 2007; (4):CD005324.
Article38. Wren TA, Lee DC, Hara R, Rethlefsen SA, Kay RM, Dorey FJ, Gilsanz V. Effect of high-frequency, low-magnitude vibration on bone and muscle in children with cerebral palsy. J Pediatr Orthop. 2010; 30:732–738.
Article39. Antoniazzi F, Monti E, Venturi G, Franceschi R, Doro F, Gatti D, Zamboni G, Tato L. GH in combination with bisphosphonate treatment in osteogenesis imperfecta. Eur J Endocrinol. 2010; 163:479–487.
Article
