Low-Tube-Voltage CT Urography Using Low-Concentration-Iodine Contrast Media and Iterative Reconstruction: A Multi-Institutional Randomized Controlled Trial for Comparison with Conventional CT Urography
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea. radjycho@snu.ac.kr
- 2Institute of Radiation Medicine and Kidney Research Institute, Seoul National University, Seoul 03080, Korea.
- 3Medical Research Collaborating Center, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea.
- 4Department of Radiology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam 13621, Korea.
- 5Department of Radiology, SMG-SNU Boramae Medical Center, Seoul National University College of Medicine, Seoul 07061, Korea.
- 6Department of Radiology, Ajou University Hospital, Ajou University School of Medicine, Suwon 16499, Korea.
- 7Department of Radiology, Soonchunhyang University Seoul Hospital, Seoul 04401, Korea.
- 8Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea.
- 9Department of Radiology, Korea University Guro Hospital, Korea University College of Medicine, Seoul 08308, Korea.
- 10Department of Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul 06973, Korea.
- 11Department of Radiology, Korea University Anam Hospital, Korea University College of Medicine, Seoul 02841, Korea.
- 12Department of Radiology, Hanyang University Guri Hospital, Guri 11923, Korea.
- 13Department of Radiology, Dankook University Hospital, Dankook University College of Medicine, Cheonan 31116, Korea.
- 14Department of Radiology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul 05030, Korea.
- 15Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea.
- 16Department of Radiology, Dong-A University College of Medicine, Busan 49201, Korea.
- 17Department of Radiology, Hallym University Sacred Heart Hospital, Anyang 14068, Korea.
- 18Department of Radiology, Gachon University, Gil Medical Center, Incheon 21565, Korea.
- 19Department of Radiology, Cheongyang-gun Health Center and County Hospital, Cheongyang 33324, Korea.
- 20Department of Radiology, Armed Forces Daejeon Hospital, Daejeon 34059, Korea.
- 21Department of Radiology, Sheikh Khalifa Specialty Hospital, Ras al Khaimah, UAE.
- KMID: 2424851
- DOI: http://doi.org/10.3348/kjr.2018.19.6.1119
Abstract
OBJECTIVE
To compare the image quality of low-tube-voltage and low-iodine-concentration-contrast-medium (LVLC) computed tomography urography (CTU) with iterative reconstruction (IR) with that of conventional CTU.
MATERIALS AND METHODS
This prospective, multi-institutional, randomized controlled trial was performed at 16 hospitals using CT scanners from various vendors. Patients were randomly assigned to the following groups: 1) the LVLC-CTU (80 kVp and 240 mgI/mL) with IR group and 2) the conventional CTU (120 kVp and 350 mgI/mL) with filtered-back projection group. The overall diagnostic acceptability, sharpness, and noise were assessed. Additionally, the mean attenuation, signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), and figure of merit (FOM) in the urinary tract were evaluated.
RESULTS
The study included 299 patients (LVLC-CTU group: 150 patients; conventional CTU group: 149 patients). The LVLC-CTU group had a significantly lower effective radiation dose (5.73 ± 4.04 vs. 8.43 ± 4.38 mSv) compared to the conventional CTU group. LVLC-CTU showed at least standard diagnostic acceptability (score ≥ 3), but it was non-inferior when compared to conventional CTU. The mean attenuation value, mean SNR, CNR, and FOM in all pre-defined segments of the urinary tract were significantly higher in the LVLC-CTU group than in the conventional CTU group.
CONCLUSION
The diagnostic acceptability and quantitative image quality of LVLC-CTU with IR are not inferior to those of conventional CTU. Additionally, LVLC-CTU with IR is beneficial because both radiation exposure and total iodine load are reduced.
MeSH Terms
Figure
-
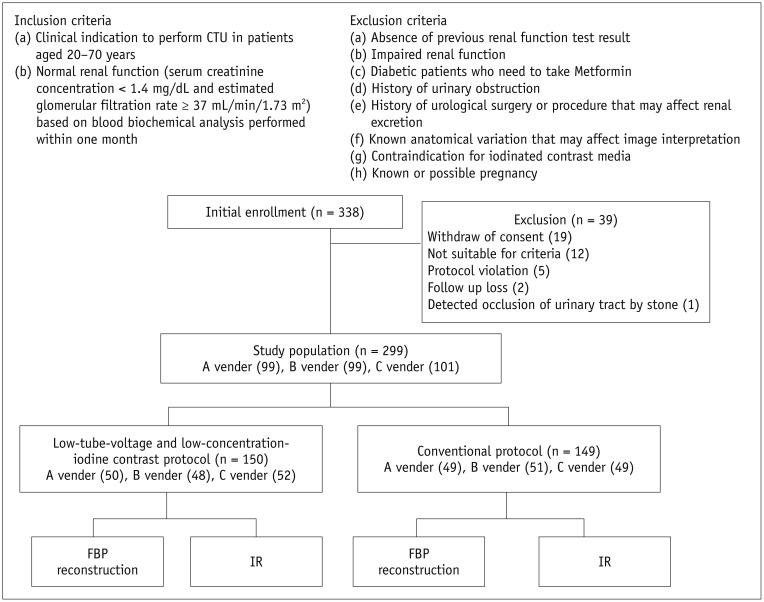
Fig. 1 Inclusion criteria, exclusion criteria, and flowchart for enrollment of study population.Nineteen patients withdrew consent prior to CTU. Twelve patients were excluded for following reasons: 1) age > 70 years (n = 4); 2) abnormal renal function test results (n = 3); 3) metformin usage (n = 3); and 4) history of urinary tract obstruction (n = 2). Additionally, 8 patients were excluded for following reasons: 1) protocol violation (n = 5); 2) follow-up loss (n = 2); and 3) limitation of image assessment owing to incidental detection of urinary tract obstruction by urinary stone (n = 1). CTU = computed tomography urography, FBP = filtered-back projection, IR = iterative reconstruction
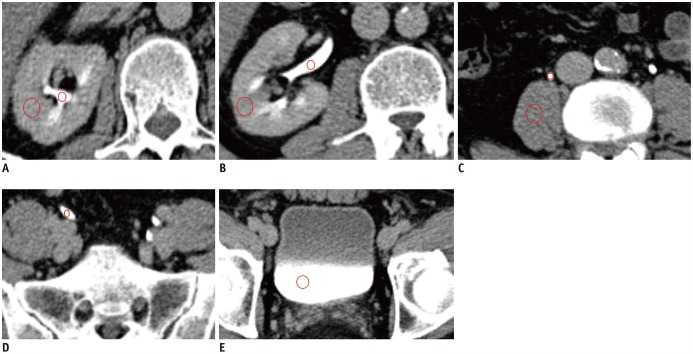
Fig. 2 Quantitative measurements of urinary tract, renal parenchyma, and psoas muscle.Mean attenuation values (HU) were measured in contrast-filled regions of urinary tract including major calyx (A), renal pelvis and parenchyma (B), upper ureter and psoas muscle (C), lower ureter (D), and urinary bladder (E) with manually drawn circular ROIs (red circles). Sizes of ROIs for contrast-filled pelvocalyces and ureters were approximately 10–20 mm2 in axial or coronal images that better visualized urinary tract. Sizes of ROIs for renal parenchyma, psoas muscle, and bladder were approximately 40–100 mm2. Care was taken to avoid vessels, prominent artifacts (i.e., streak artifacts), and heterogeneous enhancing areas in renal parenchyma (i.e., focal scarring) and to place ROI in most homogeneous area. Urinary tract was measured on both sides separately (only right side was shown). HU = Hounsfield unit, ROIs = regions of interest
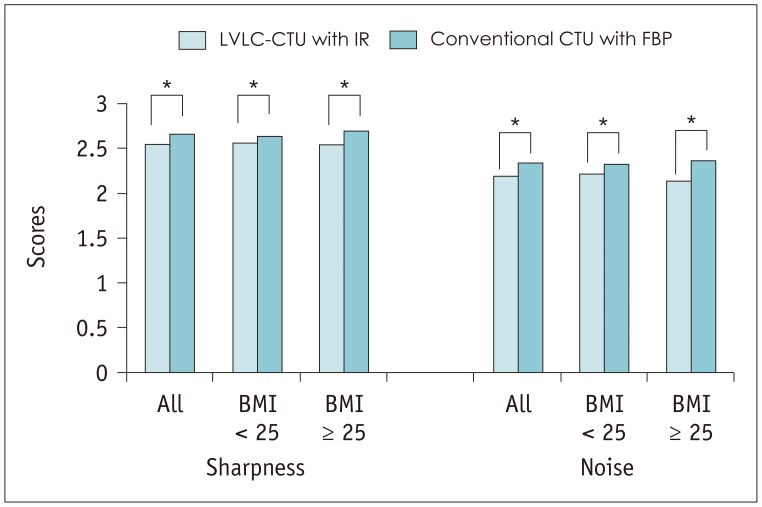
Fig. 3 Image sharpness and image noise for LVLC-CTU with IR and conventional CTU with FBP.Noise and sharpness scores for LVLC-CTU with IR (2.55 ± 0.24) were significantly lower than those for conventional CTU with FBP (2.66 ± 0.17, p < 0.001). However, LVLC-CTU with IR showed at least acceptable noise and average sharpness (score of 2). BMI = body mass index, LVLC = low-tube-voltage and low-iodine-concentration-contrast-medium
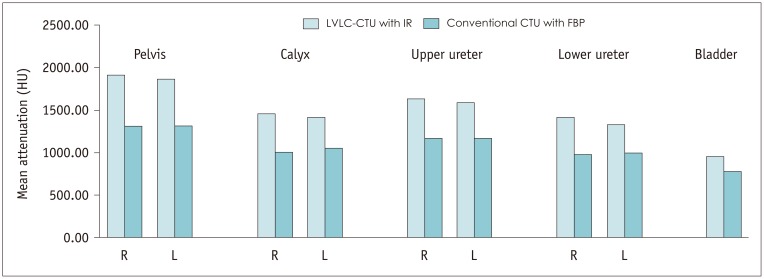
Fig. 4 Mean attenuation measured using LVLC-CTU with IR and conventional CTU with FBP.Mean attenuation value for LVLC-CTU with IR was significantly higher than that for conventional CTU with FBP in all pre-defined segments of urinary tract including pelvocalyces on both sides and urinary bladder.
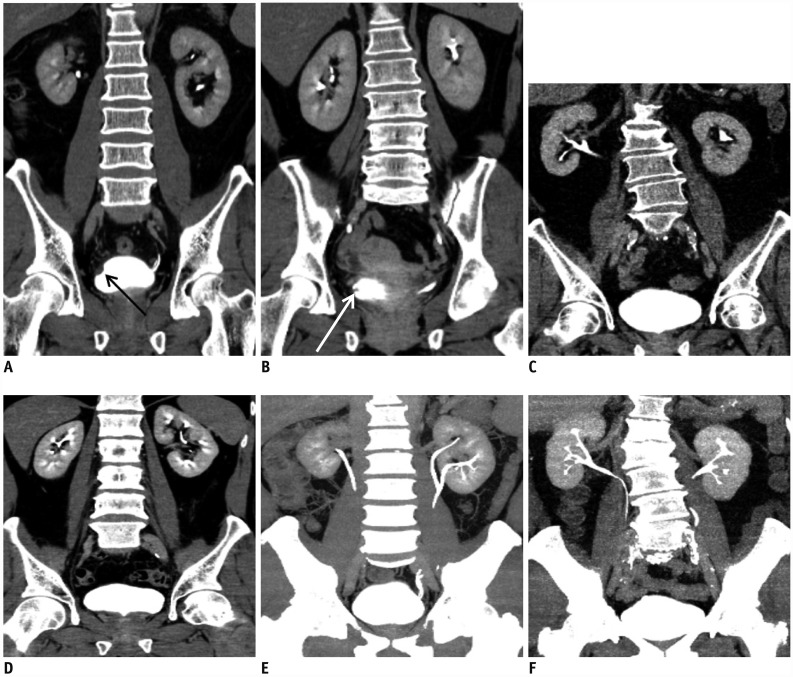
Fig. 5 Multi-planar reconstructed images of excretory phase in CTU.In conventional CTU with FBP images acquired from patients with high BMI (A) and low BMI (B), filling defects due to polypoid tumor (arrow) (A) or trabeculated muscle (arrow) (B) were well visualized with high contrast-to-noise ratio. In LVLC-CTU with IR images acquired from patients with high BMI (C) and low BMI (D), collecting systems, including calyces and urinary bladder, showed high attenuation. Diagnostic acceptability scores were comparable between two protocols. In maximum intensity projection images of urinary tract involving LVLC with IR (E) or conventional CTU with FBP (F), urinary tract was well visualized with LVLC-CTU compared to conventional CTU, despite injection of iodine contrast with low osmolality.
Reference
-
1. Silverman SG, Leyendecker JR, Amis ES Jr. What is the current role of CT urography and MR urography in the evaluation of the urinary tract? Radiology. 2009; 250:309–323. PMID: 19188307.
Article2. Nawfel RD, Judy PF, Schleipman AR, Silverman SG. Patient radiation dose at CT urography and conventional urography. Radiology. 2004; 232:126–132. PMID: 15220498.
Article3. Yanaga Y, Awai K, Funama Y, Nakaura T, Hirai T, Roux S, et al. Low-dose MDCT urography: feasibility study of low-tube-voltage technique and adaptive noise reduction filter. AJR Am J Roentgenol. 2009; 193:W220–W229. PMID: 19696263.
Article4. Juri H, Matsuki M, Inada Y, Tsuboyama T, Kumano S, Azuma H, et al. Low-dose computed tomographic urography using adaptive iterative dose reduction 3-dimensional: comparison with routine-dose computed tomography with filtered back projection. J Comput Assist Tomogr. 2013; 37:426–431. PMID: 23674016.5. Kekelidze M, Dwarkasing RS, Dijkshoorn ML, Sikorska K, Verhagen PC, Krestin GP. Kidney and urinary tract imaging: triple-bolus multidetector CT urography as a one-stop shop--protocol design, opacification, and image quality analysis. Radiology. 2010; 255:508–516. PMID: 20160002.
Article6. Seyal AR, Arslanoglu A, Abboud SF, Sahin A, Horowitz JM, Yaghmai V. CT of the abdomen with reduced tube voltage in adults: a practical approach. Radiographics. 2015; 35:1922–1939. PMID: 26473536.
Article7. Nakaura T, Nakamura S, Maruyama N, Funama Y, Awai K, Harada K, et al. Low contrast agent and radiation dose protocol for hepatic dynamic CT of thin adults at 256-detector row CT: effect of low tube voltage and hybrid iterative reconstruction algorithm on image quality. Radiology. 2012; 264:445–454. PMID: 22627597.
Article8. Namimoto T, Oda S, Utsunomiya D, Shimonobo T, Morita S, Nakaura T, et al. Improvement of image quality at low-radiation dose and low-contrast material dose abdominal CT in patients with cirrhosis: intraindividual comparison of low tube voltage with iterative reconstruction algorithm and standard tube voltage. J Comput Assist Tomogr. 2012; 36:495–501. PMID: 22805682.9. Gonzalez-Guindalini FD, Ferreira Botelho MP, Töre HG, Ahn RW, Gordon LI, Yaghmai V. MDCT of chest, abdomen, and pelvis using attenuation-based automated tube voltage selection in combination with iterative reconstruction: an intrapatient study of radiation dose and image quality. AJR Am J Roentgenol. 2013; 201:1075–1082. PMID: 24147478.
Article10. Nakayama Y, Awai K, Funama Y, Hatemura M, Imuta M, Nakaura T, et al. Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology. 2005; 237:945–951. PMID: 16237140.
Article11. Nakaura T, Awai K, Maruyama N, Takata N, Yoshinaka I, Harada K, et al. Abdominal dynamic CT in patients with renal dysfunction: contrast agent dose reduction with low tube voltage and high tube current-time product settings at 256-detector row CT. Radiology. 2011; 261:467–476. PMID: 21852567.
Article12. Gruberg L, Mintz GS, Mehran R, Gangas G, Lansky AJ, Kent KM, et al. The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre-existent chronic renal insufficiency. J Am Coll Cardiol. 2000; 36:1542–1548. PMID: 11079656.
Article13. Thomsen HS, Webb JAW. Appendix A: ESUR guidelines on contrast media version 8.1. In : Thomsen HS, Webb JAW, editors. Contrast media. 3rd ed. Berlin: Springer Berlin Heidelberg;2014. p. 257–274.14. Hwang I, Cho JY, Kim SY, Oh SJ, Ku JH, Lee J, et al. Low tube voltage computed tomography urography using low-concentration contrast media: comparison of image quality in conventional computed tomography urography. Eur J Radiol. 2015; 84:2454–2463. PMID: 26388465.
Article15. Samei E, Dobbins JT 3rd, Lo JY, Tornai MP. A framework for optimising the radiographic technique in digital X-ray imaging. Radiat Prot Dosimetry. 2005; 114:220–229. PMID: 15933112.
Article16. Goo HW. CT radiation dose optimization and estimation: an update for radiologists. Korean J Radiol. 2012; 13:1–11. PMID: 22247630.
Article17. Rouprêt M, Babjuk M, Compérat E, Zigeuner R, Sylvester RJ, Burger M, et al. European Association of Urology guidelines on upper urinary tract urothelial cell carcinoma: 2015 update. Eur Urol. 2015; 68:868–879. PMID: 26188393.
Article18. Kapoor A, Allard CB, Black P, Kassouf W, Morash C, Rendon R. Canadian guidelines for postoperative surveillance of upper urinary tract urothelial carcinoma. Can Urol Assoc J. 2013; 7:306–311. PMID: 24319507.
Article19. Kawamoto S, Fishman EK. Role of CT in postoperative evaluation of patients undergoing urinary diversion. AJR Am J Roentgenol. 2010; 194:690–696. PMID: 20173146.
Article20. Mayo-Smith WW, Hara AK, Mahesh M, Sahani DV, Pavlicek W. How I do it: managing radiation dose in CT. Radiology. 2014; 273:657–672. PMID: 25420167.
Article21. Desai GS, Fuentes Orrego JM, Kambadakone AR, Sahani DV. Performance of iterative reconstruction and automated tube voltage selection on the image quality and radiation dose in abdominal CT scans. J Comput Assist Tomogr. 2013; 37:897–903. PMID: 24270111.
Article22. Kim M, Lee JM, Yoon JH, Son H, Choi JW, Han JK, et al. Adaptive iterative dose reduction algorithm in CT: effect on image quality compared with filtered back projection in body phantoms of different sizes. Korean J Radiol. 2014; 15:195–204. PMID: 24644409.
Article23. Desai GS, Uppot RN, Yu EW, Kambadakone AR, Sahani DV. Impact of iterative reconstruction on image quality and radiation dose in multidetector CT of large body size adults. Eur Radiol. 2012; 22:1631–1640. PMID: 22527370.
Article24. Yu L, Li H, Fletcher JG, McCollough CH. Automatic selection of tube potential for radiation dose reduction in CT: a general strategy. Med Phys. 2010; 37:234–243. PMID: 20175486.
Article25. Wang X, He W, Chen J, Hu Z, Zhao L. Feasibility study of radiation dose reduction in adult female pelvic CT scan with low tube-voltage and adaptive statistical iterative reconstruction. Korean J Radiol. 2015; 16:1047–1055. PMID: 26357499.
Article26. Kalender WA, Deak P, Kellermeier M, van Straten M, Vollmar SV. Application- and patient size-dependent optimization of x-ray spectra for CT. Med Phys. 2009; 36:993–1007. PMID: 19378760.
Article27. Kaza RK, Platt JF, Goodsitt MM, Al-Hawary MM, Maturen KE, Wasnik AP, et al. Emerging techniques for dose optimization in abdominal CT. Radiographics. 2014; 34:4–17. PMID: 24428277.
Article28. Bae KT. Intravenous contrast medium administration and scan timing at CT: considerations and approaches. Radiology. 2010; 256:32–61. PMID: 20574084.
Article29. Caoili EM, Inampudi P, Cohan RH, Ellis JH. Optimization of multi-detector row CT urography: effect of compression, saline administration, and prolongation of acquisition delay. Radiology. 2005; 235:116–123. PMID: 15716388.
Article30. Davenport MS, Khalatbari S, Cohan RH, Dillman JR, Myles JD, Ellis JH. Contrast material-induced nephrotoxicity and intravenous low-osmolality iodinated contrast material: risk stratification by using estimated glomerular filtration rate. Radiology. 2013; 268:719–728. PMID: 23579046.
Article31. Wang ZJ, Coakley FV, Fu Y, Joe BN, Prevrhal S, Landeras LA, et al. Renal cyst pseudoenhancement at multidetector CT: what are the effects of number of detectors and peak tube voltage? Radiology. 2008; 248:910–916. PMID: 18632527.
Article32. Cho ES, Yu JS, Ahn JH, Kim JH, Chung JJ, Lee HK, et al. CT angiography of the renal arteries: comparison of lower-tube-voltage CTA with moderate-concentration iodinated contrast material and conventional CTA. AJR Am J Roentgenol. 2012; 199:96–102. PMID: 22733899.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- GB Opacification at CT by Contrast Media Injected a Few Hours Earlier in Adult with Normal Renal Function
- Is excretory urography necessary in the staging work-up of uterine cervical carcinoma?
- Effects of Iterative Reconstruction Algorithm, Automatic Exposure Control on Image Quality, and Radiation Dose: Phantom Experiments with Coronary CT Angiography Protocols
- A Comparative study of Excretory Urography and Renal Isotope Scanning on Renal Trauma
- Multidetector CT Urography in Imaging of the Urinary Tract in Patients with Hematuria
