Causes and Trauma Apportionment Score of Chronic Subdural Hematoma
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. ksleens@sch.ac.kr
- KMID: 2424314
- DOI: http://doi.org/10.13004/kjnt.2018.14.2.61
Abstract
OBJECTIVE
The pathophysiology of chronic subdural hematoma (CSH) is not yet clear. Trauma alone is not sufficient to result in CSH in young individuals, while a trivial injury can result in CSH in older adults. Although the causality and apportionment of trauma are important issues in CSH, especially in terms of insurance, it is too obscure to solve all struggles.
METHODS
There are three key factors for producing CSH. First, CSH necessitates a potential subdural reservoir. Other important precipitating factors are trauma and coagulopathy. However, these factors are not sufficient to cause CSH development. The trauma apportionment score (TAS) can be used to compare the relative importance of these three factors. Here, we applied the TAS to 239 consecutive cases of CSH. We retrospectively obtained the patients' history and laboratory results from their medical records.
RESULTS
The TAS ranged from −5 to 5. The most common score was 0. If we defined the cause of CSH as being combined when the TAS was 0, then the cause was combined in 30 cases (12.6%). If we extended the criteria for a combined cause from 0 to −1 to 1, the cause was combined in 107 cases (44.8%). Regardless of the criteria used, traumatic CSHs were more common than were spontaneous CSHs. Spontaneous CSHs were more common in older than in younger patients (p < 0.01, Fisher's exact test).
CONCLUSION
The TAS is a useful tool for differentiating the causality of CSH.
Keyword
MeSH Terms
Figure
-
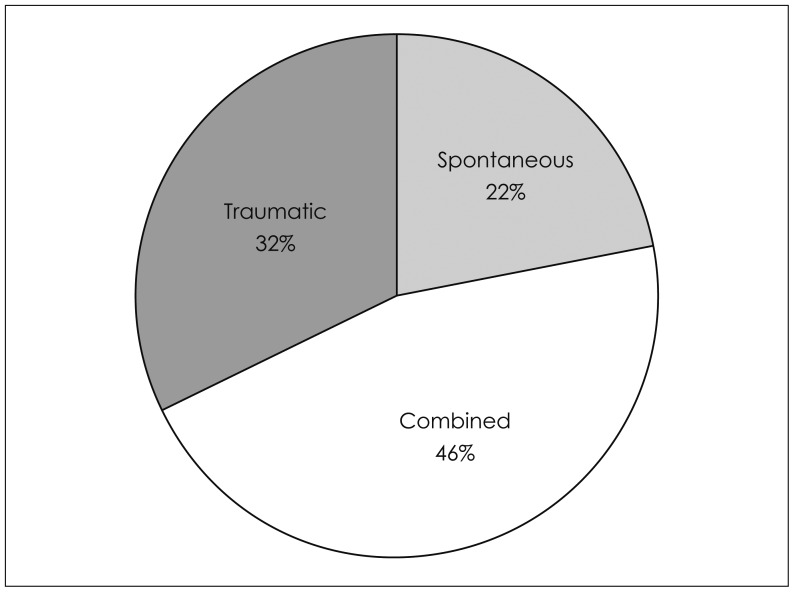
FIGURE 1 Distribution of the estimated causes of 239 cases of chronic subdural hematomas. When the trauma apportionment score is −1 to 1, the cause is regarded as combined. This extended criteria may be suitable for a legal judgment or an economical estimation.
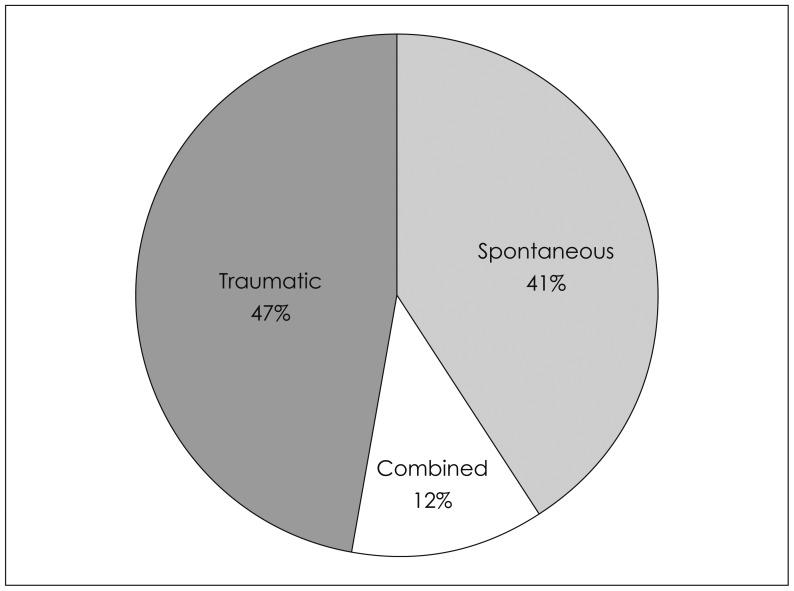
FIGURE 2 Distribution of the estimated causes of 239 cases of chronic subdural hematomas. When the trauma apportionment score is 0, the cause is regarded as combined. This narrow criteria may be a useful tool for medical or academical study.
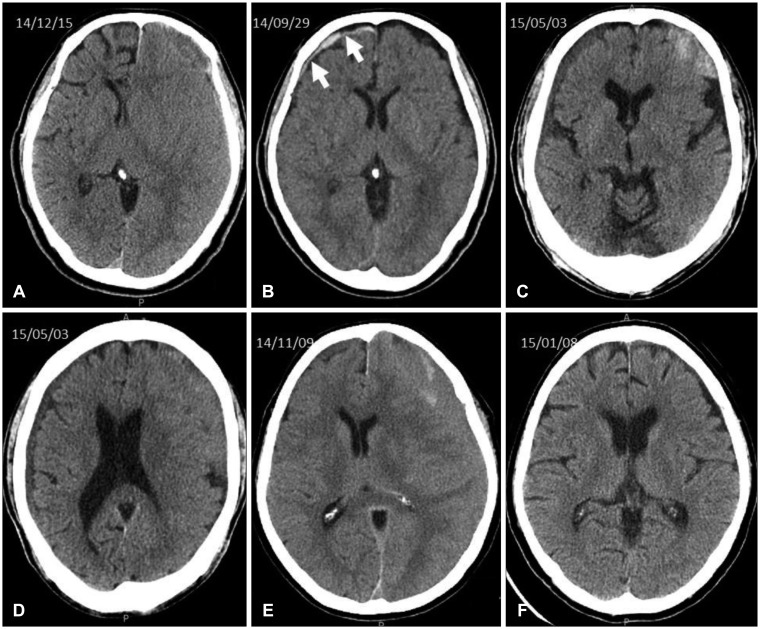
FIGURE 3 Computed tomography scans of Case 1 to 3. A chronic subdural hematoma (A) was developed on the opposite side of the acute subdural hematoma (B) after trauma in Case 1. Bilateral hematomas (C, D) were found in Case 2. Isodense chronic subdural hematoma on the left side (E) was resolved after a burr-hole drainage (F) in Case 3.
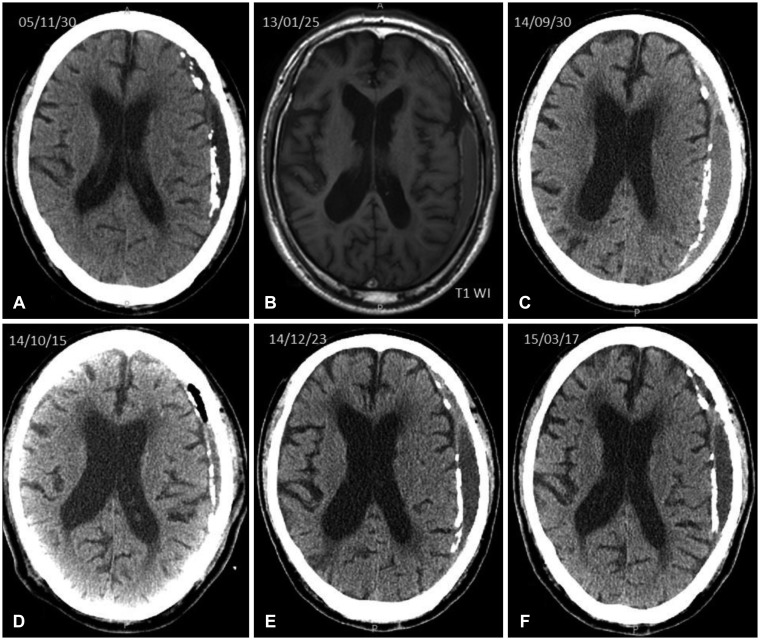
FIGURE 4 Computed tomography scans and magnetic resonance imaging of Case 4. Chronic subdural hematoma with calcification was evacuated by a burr-hole on October 2014 (D), however it remained over almost 10 years.
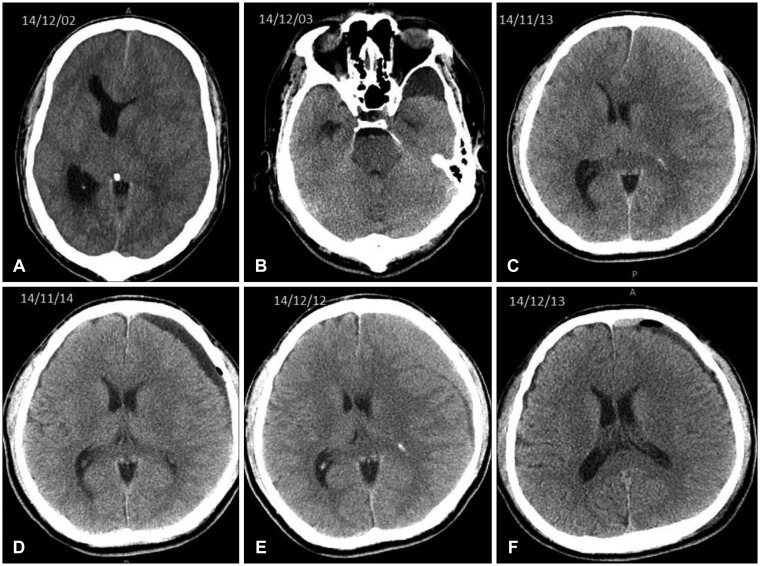
FIGURE 5 Computed tomography scans of Case 5 and 6. An arachnoid cyst on the left temporal pole (B) was noticed after burr-hole drainage of the chronic subdural hematoma on the same side (A) in Case 5. An isodense chronic subdural hematoma (C) were drained by a burr-hole (D) in Case 6. However, it recurred on the same side (E). The hematoma was resolved after a burr-hole drainage (F).
Reference
-
1. Adhiyaman V, Asghar M, Ganeshram KN, Bhowmick BK. Chronic subdural haematoma in the elderly. Postgrad Med J. 2002; 78:71–75. PMID: 11807186.2. Aspegren OP, Astrand R, Lundgren MI, Romner B. Anticoagulation therapy a risk factor for the development of chronic subdural hematoma. Clin Neurol Neurosurg. 2013; 115:981–984. PMID: 23128014.
Article3. Balser D, Farooq S, Mehmood T, Reyes M, Samadani U. Actual and projected incidence rates for chronic subdural hematomas in United States Veterans Administration and civilian populations. J Neurosurg. 2015; 123:1209–1215. PMID: 25794342.
Article4. Beck J, Gralla J, Fung C, Ulrich CT, Schucht P, Fichtner J, et al. Spinal cerebrospinal fluid leak as the cause of chronic subdural hematomas in nongeriatric patients. J Neurosurg. 2014; 121:1380–1387. PMID: 25036203.
Article5. Cheng SY, Chang CK, Chen SJ, Lin JF, Tsai CC. Chronic subdural hematoma in elderly Taiwan patients: A retrospective analysis of 342 surgical cases. Int J Gerontol. 2014; 8:37–41.
Article6. D'Errico AP, German WJ. Chronic subdural hematoma. Yale J Biol Med. 1930; 3:11–20. PMID: 21433469.7. De Bonis P, Trevisi G, de Waure C, Sferrazza A, Volpe M, Pompucci A, et al. Antiplatelet/anticoagulant agents and chronic subdural hematoma in the elderly. PLoS One. 2013; 8:e68732. PMID: 23874740.
Article8. Fjell AM, Westlye LT, Amlien I, Espeseth T, Reinvang I, Raz N, et al. High consistency of regional cortical thinning in aging across multiple samples. Cereb Cortex. 2009; 19:2001–2012. PMID: 19150922.
Article9. Fogelholm R, Heiskanen O, Waltimo O. Chronic subdural hematoma in adults. Influence of patient's age on symptoms, signs, and thickness of hematoma. J Neurosurg. 1975; 42:43–46. PMID: 1167376.10. Forster MT, Mathe AK, Senft C, Scharrer I, Seifert V, Gerlach R. The influence of preoperative anticoagulation on outcome and quality of life after surgical treatment of chronic subdural hematoma. J Clin Neurosci. 2010; 17:975–979. PMID: 20580997.
Article11. Lee KS. Natural history of chronic subdural haematoma. Brain Inj. 2004; 18:351–358. PMID: 14742149.12. Lee KS, Bae WK, Doh JW, Bae HG, Yun IG. Origin of chronic subdural haematoma and relation to traumatic subdural lesions. Brain Inj. 1998; 12:901–910. PMID: 9839025.13. Lindvall P, Koskinen LO. Anticoagulants and antiplatelet agents and the risk of development and recurrence of chronic subdural haematomas. J Clin Neurosci. 2009; 16:1287–1290. PMID: 19564115.
Article14. Markwalder TM. Chronic subdural hematomas: a review. J Neurosurg. 1981; 54:637–645. PMID: 7014792.
Article15. Mori K, Maeda M. Surgical treatment of chronic subdural hematoma in 500 consecutive cases: clinical characteristics, surgical outcome, complications, and recurrence rate. Neurol Med Chir (Tokyo). 2001; 41:371–381. PMID: 11561347.
Article16. Park HR, Lee KS, Shim JJ, Yoon SM, Bae HG, Doh JW. Multiple densities of the chronic subdural hematoma in CT scans. J Korean Neurosurg Soc. 2013; 54:38–41. PMID: 24044079.
Article17. Sim YW, Min KS, Lee MS, Kim YG, Kim DH. Recent changes in risk factors of chronic subdural hematoma. J Korean Neurosurg Soc. 2012; 52:234–239. PMID: 23115667.
Article18. Soleman J, Taussky P, Fandino J, Muroi C. Evidence-based treatment of chronic subdural hematoma. Rijeka, HR: Intech;2014. Accessed December 10, 2016. http://www.intechopen.com/books/traumatic-brain-injury/evidence-based-treatment-of-chronic-subdural-hematoma.19. Sousa EB, Brandao LF, Tavares CB, Borges IB, Neto NG, Kessler IM. Epidemiological characteristics of 778 patients who underwent surgical drainage of chronic subdural hematomas in Brasilia, Brazil. BMC Surg. 2013; 13:5. PMID: 23452673.
Article20. Walhovd KB, Westlye LT, Amlien I, Espeseth T, Reinvang I, Raz N, et al. Consistent neuroanatomical age-related volume differences across multiple samples. Neurobiol Aging. 2011; 32:916–932. PMID: 19570593.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
- Chronic Subdural Hematoma Due to Cumulative Trauma to the Head
- Bilateral Acute Subdural Hematoma Following Evacuation of Chronic Subdural Hematoma
- Arachnoid Cyst with Spontaneous Intracystic Hemorrhage and Chronic Subdural Hematoma
- Intraoperative Development of Contralateral Subdural Hematoma during Evacuation of Acute Subdural Hematoma: Case Report
