Arachnoid Granulations Mimicking Multiple Osteolytic Bone Lesions in the Occipital Bone
- Affiliations
-
- 1Department of Neurosurgery, Kyungpook National University School of Medicine, Kyungpook National University Hospital, Daegu, Korea. nsdoctor@naver.com
- KMID: 2423976
- DOI: http://doi.org/10.14791/btrt.2018.6.e8
Abstract
- We report a rare case of arachnoid granulations mimicking multiple osteolytic bone lesions. A 66-year-old woman was admitted to a local clinic for a regular checkup. Upon admission, brain CT showed multiple osteolytic lesions in the occipital bone. These needed to be differentiated from multiple osteolytic bone tumor. Subsequent brain MRI revealed that the osteolytic lesions were isointense to cerebrospinal fluid, hyperintense on T2-weighted image, hypointense on T1-weighted image, and with subtle capsules around the osteolytic lesions that were visible after gadolinium injection. A bone scan revealed no radiotracer uptake. The lesions were in both the transverse sinuses and the torcular herophili. With typical radiological appearances of the lesions, the osteolytic lesions were diagnosed as multiple arachnoid granulations. No further treatment was planned. A 1-year follow-up brain CT scan revealed no change. We should consider the possibility of arachnoid granulations when multiple osteolytic lesions are observed in the occipital bone.
Keyword
MeSH Terms
Figure
-

Fig. 1 Lateral (A) and Townes (B) skull X-rays show multiple osteolytic lesions in the occipital bone without apparent sclerotic margins.
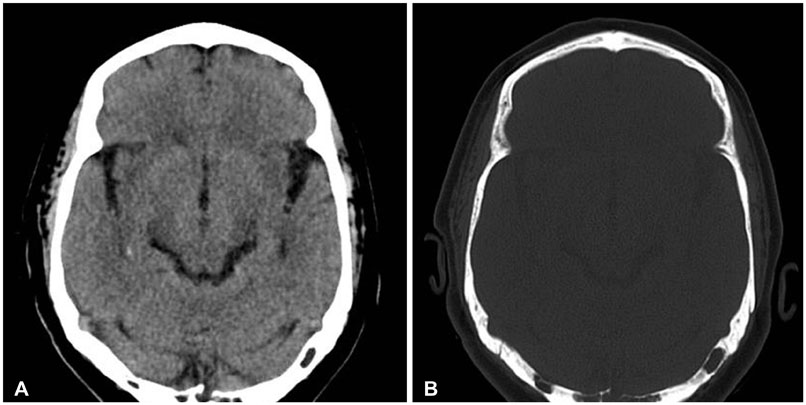
Fig. 2 Brain CT scans on soft-tissue windows (A) and bone windows (B) show multiple osteolytic lesions in the occipital bone around both the transverse sinuses and the torcular herophili, involving both the inner and outer tables.
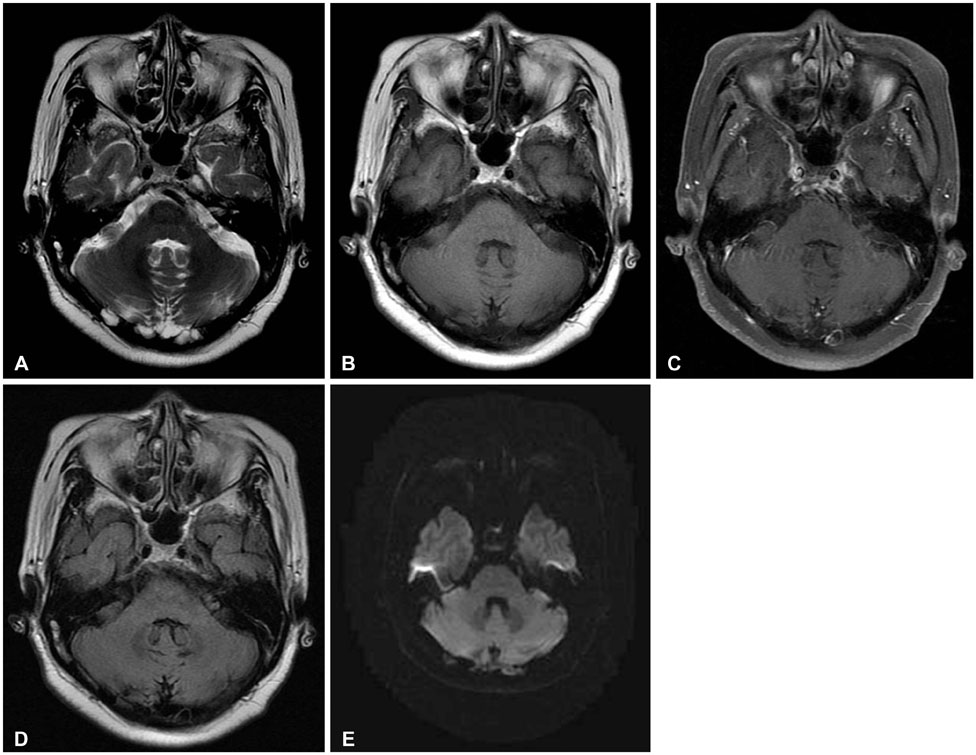
Fig. 3 Brain MRI images reveal a high signal intensity on T2-weighted image (A), a low signal intensity on T1-weighted image (B) and subtle capsules around lesions that are visible after gadolinium injection (C), complete suppression on fluid attenuated inversion recovery image (D), and no restricted diffusion on diffusion-weighted imaging (E).

Fig. 4 Whole body bone scan with 99mTc-hydroxy diphosphonate shows no increased radiotracer uptake.
Reference
-
1. Kan P, Stevens EA, Couldwell WT. Incidental giant arachnoid granulation. AJNR Am J Neuroradiol. 2006; 27:1491–1492.2. Branan R, Wilson CB. Arachnoid granulations simulating osteolytic lesions of the calvarium. AJR Am J Roentgenol. 1976; 127:523–525.
Article3. Watane GV, Patel B, Brown D, Taheri MR. The significance of arachnoid granulation in patients with idiopathic intracranial hypertension. J Comput Assist Tomogr. 2018; 42:282–285.
Article4. Trimble CR, Harnsberger HR, Castillo M, Brant-Zawadzki M, Osborn AG. “Giant” arachnoid granulations just like CSF?: NOT!! AJNR Am J Neuroradiol. 2010; 31:1724–1728.
Article5. Amlashi SF, Riffaud L, Morandi X. Intracranial hypertension and giant arachnoid granulations. J Neurol Neurosurg Psychiatry. 2004; 75:172–174.6. Leach JL, Meyer K, Jones BV, Tomsick TA. Large arachnoid granulations involving the dorsal superior sagittal sinus: findings on MR imaging and MR venography. AJNR Am J Neuroradiol. 2008; 29:1335–1339.
Article7. Ikushima I, Korogi Y, Makita O, et al. MRI of arachnoid granulations within the dural sinuses using a FLAIR pulse sequence. Br J Radiol. 1999; 72:1046–1051.
Article8. Haroun AA, Mahafza WS, Al Najar MS. Arachnoid granulations in the cerebral dural sinuses as demonstrated by contrast-enhanced 3D magnetic resonance venography. Surg Radiol Anat. 2007; 29:323–328.
Article9. Koshikawa T, Naganawa S, Fukatsu H, Ishiguchi T, Ishigaki T. Arachnoid granulations on high-resolution MR images and diffusion-weighted MR images: normal appearance and frequency. Radiat Med. 2000; 18:187–191.10. Lu CX, Du Y, Xu XX, et al. Multiple occipital defects caused by arachnoid granulations: emphasis on T2 mapping. World J Radiol. 2012; 4:341–344.
Article11. Kiroglu Y, Yaqci B, Cirak B, Karabulut N. Giant arachnoid granulation in a patient with benign intracranial hypertension. Eur Radiol. 2008; 18:2329–2332.
Article12. VandeVyver V, Lemmerling M, De Foer B, Casselman J, Verstraete K. Arachnoid granulations of the posterior temporal bone wall: imaging appearance and differential diagnosis. AJNR Am J Neuroradiol. 2007; 28:610–612.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant Arachnoid Granulations in Headache Mimicking Migraine with Aura
- Metastatic breast cancer with osteolytic skull lesions suspected to be multiple myeloma
- Subchondral Bone Restoration of Supra-acetabular Brown Tumor Secondary to Parathyroid Carcinoma: A Case Report
- Symptomatic Benign Intraosseous Osteolytic Lesions of the Glenoid: Report of 3 cases
- A case report of aneurysmal bone cyst in involving occipital bone
