Pulmonary Extraintestinal Manifestation of Crohn's Disease Treated Successfully with Adalimumab
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea. cho6706@hanmail.net
- 2Department of Pathology, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- 3Department of Radiology, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- KMID: 2420752
- DOI: http://doi.org/10.4166/kjg.2018.72.3.141
Abstract
- Pulmonary extraintestinal manifestation is rare in Crohn's disease and has been reported in only a few cases. Despite the presence of pulmonary abnormalities in a significant proportion of patients with inflammatory bowel disease, there are only few case reports, due to complicated diagnosis and low recognition by clinicians. Currently, treatment guidelines for pulmonary Crohn's disease have not been established. There are some case reports of pulmonary Crohn's disease that achieved remission after infliximab treatment. Clinical and radiological remission of pulmonary extraintestinal involvement in Crohn's disease after adalimumab therapy has not been reported yet. Here, we report one case of lung involvement of Crohn's disease, which shows radiological and clinical remission after adalimumab treatment.
Keyword
MeSH Terms
Figure
-

Fig. 1 Chest CT findings revealed multiple ill-defined pulmonary nodules (arrows) in bilateral lung fields. CT, computed tomography.

Fig. 2 Colonoscopy findings showing multiple various sized longitudinal ulcers and perianal ulcers with edematous changes.

Fig. 3 PET-CT showed multiple various sized ill-defined pulmonary nodules (arrows) with highly increased 18F-FDG uptake (pSUV 3.67–8.88). PET, positron emission tomography; CT, computed tomography; 18F-FDG, fluorine-18 fluorodeoxyglucose; pSUV, peak standardized uptake value.
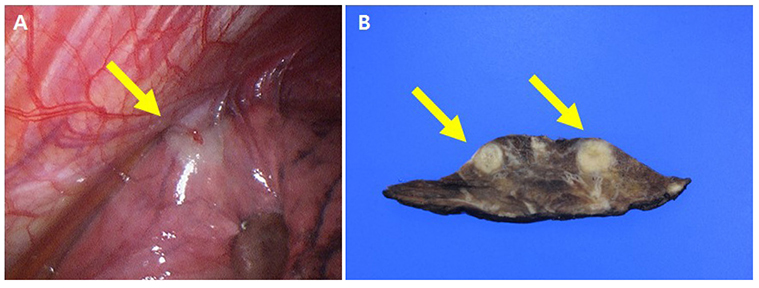
Fig. 4 (A) The surgical field observed by video-assisted thoracoscopy showing whitish mucous patch-like lesion (arrow). (B) Two ill-demarcated necrotic lesions (arrows) are shown on gross photograph after thoracic wedge resection.
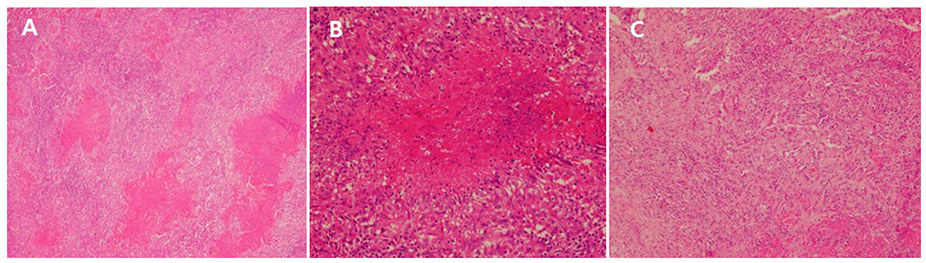
Fig. 5 (A) Prominent parenchymal geographical necrosis is observed (H&E, ×40). (B) Necrotizing granuloma (H&E, ×200). (C) Organizing pneumonia involving lung parenchyma (H&E, ×100).
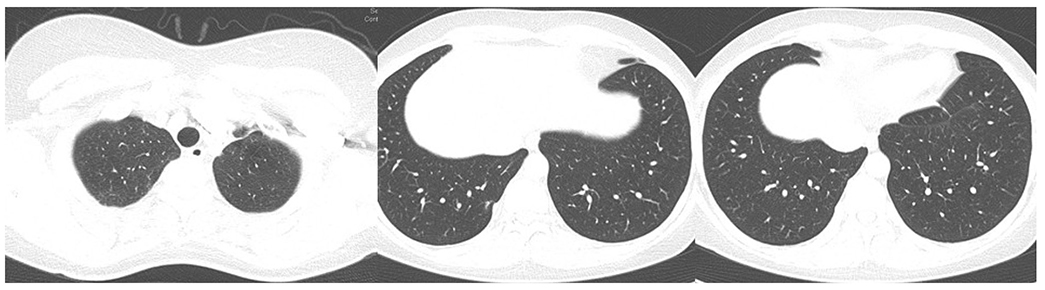
Fig. 6 Significantly decreased previous lung nodules noted on follow-up chest CT findings. CT, computed tomography.
Reference
-
1. Lakatos PL, Lakatos L, Kiss LS, Peyrin-Biroulet L, Schoepfer A, Vavricka S. Treatment of extraintestinal manifestations in inflammatory bowel disease. Digestion. 2012; 86:Suppl 1. 28–35.
Article2. Chew MT, Chak E, Matsukuma K. A rare cause of pulmonary nodules. Case Rep Gastroenterol. 2016; 10:633–639.
Article3. Hayek AJ, Pfanner TP, White HD. Inflammatory bowel disease of the lung: the role of infliximab? Respir Med Case Rep. 2015; 15:85–88.
Article4. Black H, Mendoza M, Murin S. Thoracic manifestations of inflammatory bowel disease. Chest. 2007; 131:524–532.
Article5. Songür N, Songür Y, Tüzün M, et al. Pulmonary function tests and high-resolution CT in the detection of pulmonary involvement in inflammatory bowel disease. J Clin Gastroenterol. 2003; 37:292–298.6. Vutcovici M, Brassard P, Bitton A. Inflammatory bowel disease and airway diseases. World J Gastroenterol. 2016; 22:7735–7741.
Article7. Lu DG, Ji XQ, Liu X, Li HJ, Zhang CQ. Pulmonary manifestations of Crohn's disease. World J Gastroenterol. 2014; 20:133–141.
Article8. Olpin JD, Sjoberg BP, Stilwill SE, Jensen LE, Rezvani M, Shaaban AM. Beyond the bowel: extraintestinal manifestations of inflammatory bowel disease. Radiographics. 2017; 37:1135–1160.
Article9. Yoon HS, Lee EJ, Lee JY, Chon GR, Lee SH, Kim SJ. Organizing pneumonia associated with M ycobacterium tuberculosis infection. Respirol Case Rep. 2015; 3:128–131.10. Vaszar LT, Orzechowski NM, Specks U, et al. Coexistent pulmonary granulomatosis with polyangiitis (Wegener granulomatosis) and Crohn disease. Am J Surg Pathol. 2014; 38:354–359.
Article11. Majewski S, Piotrowski W. Pulmonary manifestations of inflammatory bowel disease. Arch Med Sci. 2015; 11:1179–1188.
Article12. Ardizzone S, Puttini PS, Cassinotti A, Porro GB. Extraintestinal manifestations of inflammatory bowel disease. Dig Liver Dis. 2008; 40:Suppl 2. S253–S259.
Article13. Pedersen N, Duricova D, Munkholm P. Pulmonary Crohn's disease: a rare extra-intestinal manifestation treated with infliximab. J Crohns Colitis. 2009; 3:207–211.
Article14. Camus P, Colby TV. The lung in inflammatory bowel disease. Eur Respir J. 2000; 15:5–10.
Article15. Louis EJ, Reinisch W, Schwartz DA, et al. Adalimumab reduces extraintestinal manifestations in patients with Crohn's disease: a pooled analysis of 11 clinical studies. Adv Ther. 2018; 35:563–576.
Article16. Chalhoub JM, Rimmani HH, Gumaste VV, Sharara AI. Systematic review and meta-analysis: adalimumab monotherapy versus combination therapy with immunomodulators for induction and maintenance of remission and response in patients with Crohn's disease. Inflamm Bowel Dis. 2017; 23:1316–1327.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adalimumab or infliximab: which is better for perianal fistula in Crohn's disease?
- A Case of Pulmonary Thromboembolism in Crohn's Disease
- Adalimumab Treatment in Pediatric-Onset Crohn's Disease Patients after Infliximab Failure: A Single Center Study
- Eruptive Benign Melanocytic Nevi Formation Following Adalimumab Therapy in a Patient with Crohn's Disease
- A Case of Granulomatous Liver Disease Combined with Crohn's Disease
