Yonsei Med J.
2017 May;58(3):658-661. 10.3349/ymj.2017.58.3.658.
Quarter-Shifted Microincisional Sutureless Vitrectomy in Patients with a Glaucoma Drainage Implant or Filtering Bleb
- Affiliations
-
- 1Department of Ophthalmology, Ajou University School of Medicine, Suwon, Korea. dreyesong@naver.com
- 2Kong Eye Hospital, Seoul, Korea.
- KMID: 2419127
- DOI: http://doi.org/10.3349/ymj.2017.58.3.658
Abstract
- When vitrectomy is performed in eyes that have undergone glaucoma surgery, the site of sclerotomy often overlaps with the previous glaucoma operation site. It can lead to serious complications such as postoperative hypotony, leakage, and/or infection. Our technique involves modification of surgeon's position and two sclerotomy sites 45° away from the original position, with an infusion cannula inserted infranasally to avoid damage to the glaucoma drainage implant or filtering bleb. The modified approach was applied to seven eyes with various indications. Vitrectomy was successfully completed, and there were no sclerotomy site complications, leakage, or hypotony in any case. Good intraocular pressure control was maintained throughout the postoperative course in all cases.
MeSH Terms
Figure
-
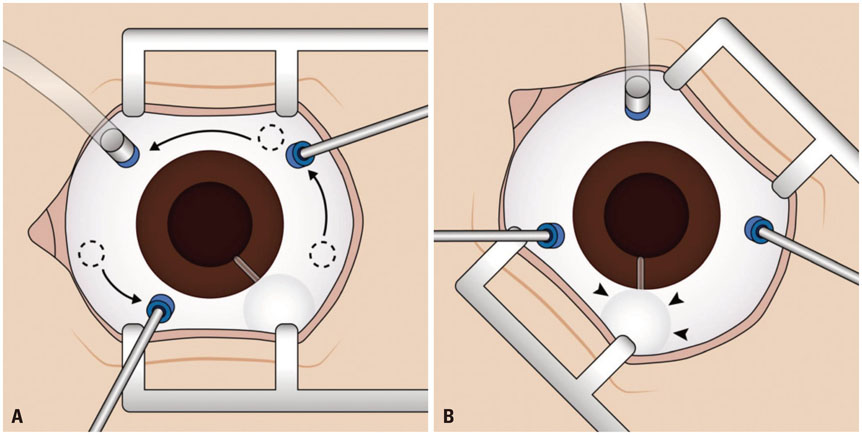
Fig. 1 Surgical technique of quarter-shifted vitrectomy. (A) Conventional sites of the three sclerotomy incisions (dotted circle) are displaced. First, the infusion cannula is moved to the infranasal side. Second, the other two incision sites are shifted to a 45°-counterclockwise position, away from the original sites (arrows). (B) Changed surgeon's view of a supratemporally positioned vitrectomy. The glaucoma drainage implants are located away from the vitrectomy cannulas and are therefore undamaged (arrowheads).
Reference
-
1. Ryan EH Jr, Gilbert HD. Lensectomy, vitrectomy indications, and techniques in cataract surgery. Curr Opin Ophthalmol. 1996; 7:69–74.
Article2. Peyman GA, Carney MD, Higginbotham EJ. Lensectomy and vitrectomy in the presence of filtering blebs. Int Ophthalmol. 1987; 10:143–147.
Article3. Kunikata H, Aizawa N, Fuse N, Abe T, Nakazawa T. 25-gauge microincision vitrectomy to treat vitreoretinal disease in glaucomatous eyes after trabeculectomy. J Ophthalmol. 2014; 2014:306814.
Article4. Closa RC, Pereira LS, Lam HH, Stewart JM. Pars plana vitrectomy from a temporal approach for a patient with a deep orbit. Retin Cases Brief Rep. 2009; 3:212–213.
Article5. Tarantola RM, Graff JM, Somani R, Mahajan VB. Temporal approach for small-gauge pars plana vitrectomy combined with anterior segment surgery. Retina. 2012; 32:1614–1623.
Article6. Miki M, Ueki M, Sugiyama T, Kojima S, Ikeda T. A case involving an Ahmed™ glaucoma valve transferred from the vitreous into the anterior chamber of the eye with a silicone oil tamponade for the treatment of neovascular glaucoma. Clin Ophthalmol. 2013; 7:449–453.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Use of e-PTFE Membrane for Glaucoma Drainage Surgery
- The Comparative Assessment of Filtering Bleb by Timing of subconjunctival Injection of Mitomycin-C in Glaucoma Filtering Surgery
- 5-Fluorouracil in a Collagen Sponge and Glaucoma Filtering Surgery
- A membranous drainage implant in glaucoma filtering surgery: animal trial
- Triamcinolone and Glaucoma Filtering Surgery
