Protein-Losing Enteropathy as a Complication of the Ketogenic Diet
- Affiliations
-
- 1Division of Pediatric Neurology, Department of Pediatrics, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea. hdkimmd@yuhs.ac
- 2Department of Pediatrics, College of Medicine, Soonchunhyang University, Bucheon Hospital, Bucheon, Korea.
- KMID: 2419101
- DOI: http://doi.org/10.3349/ymj.2017.58.4.891
Abstract
- The ketogenic diet is an effective treatment for the patients with intractable epilepsy, however, the diet therapy can sometimes be discontinued by complications. Protein-losing enteropathy is a rarely reported serious complication of the ketogenic diet. We present a 16-month-old Down syndrome baby with protein-losing enteropathy during the ketogenic diet as a treatment for West syndrome. He suffered from diarrhea, general edema and hypoalbuminemia which were not controlled by conservative care for over 1 month. Esophagogastroduodenoscopy and stool alpha-1 antitrypsin indicated protein-losing enteropathy. Related symptoms were relieved after cessation of the ketogenic diet. Unexplained hypoalbuminemia combined with edema and diarrhea during ketogenic suggests the possibility of protein-losing enteropathy, and proper evaluation is recommended in order to expeditiously detect it and to act accordingly.
MeSH Terms
Figure
-
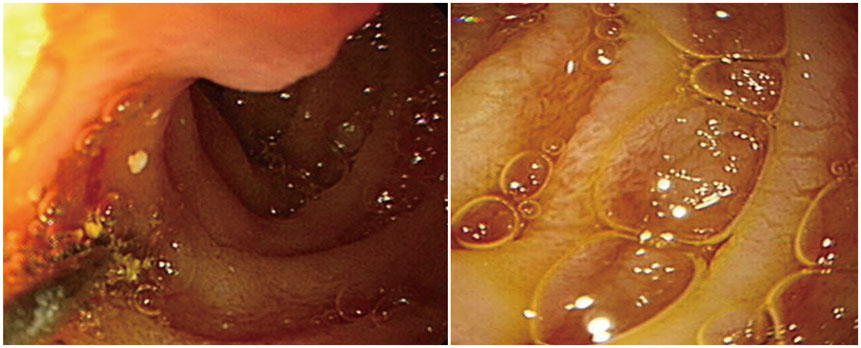
Fig. 1 Edematous mucosa and some whitish patches were noted on the duodenum. Slightly edematous gastric mucosa was also noted. Biopsies were acquired from the duodenum and the stomach. Pathology result: ectatic lymphatics in lamina propria, suspicious for intestinal lymphangiectasia.
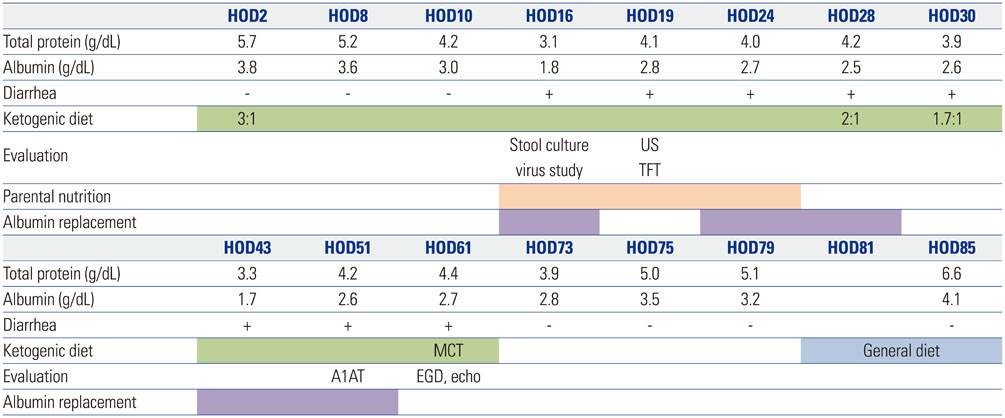
Fig. 2 Scheme of ketogenic diet, nutritional support, evaluation and laboratory data. On HOD2, the ketogenic diet (3:1, fat:non-fat) was started. diarrhea and hypoalbuminemia occurred. through laboratory test, we checked normal renal function, liver function, normal flora in stool culture and noroviral infection confirmed in viral study on HOD16. And parental nutrition and albumin replacement were started. abdominal ultrasonography and thyroid function test were normal on HOD19. On HOD28, the ketogenic diet was reduced from 3:1 to 1.7:1. The symptoms were persistent, and after EGD and echocardiography on HOD61, the ketogenic diet was stopped, and a MCT was started. HOD, hospitalization day; US, abdominal ultrasonography; TFT, thyroid function test; MCT, medium chain triglycerides; A1AT, alpha-1 antitrympsin; EGD, endoscopic gastroduodenoscopy; echo, echocardiography; MCT, medium chain triglyceride diet.
Reference
-
1. DiMario FJ Jr, Holland J. The ketogenic diet: a review of the experience at Connecticut Children's Medical Center. Pediatr Neurol. 2002; 26:288–292.
Article2. Kang HC, Kim YJ, Kim DW, Kim HD. Efficacy and safety of the ketogenic diet for intractable childhood epilepsy: Korean multicentric experience. Epilepsia. 2005; 46:272–279.
Article3. Suo C, Liao J, Lu X, Fang K, Hu Y, Chen L, et al. Efficacy and safety of the ketogenic diet in Chinese children. Seizure. 2013; 22:174–178.
Article4. Kang HC, Chung DE, Kim DW, Kim HD. Early- and late-onset complications of the ketogenic diet for intractable epilepsy. Epilepsia. 2004; 45:1116–1123.
Article5. Moriyama K, Watanabe M, Yamada Y, Shiihara T. Protein-losing enteropathy as a rare complication of the ketogenic diet. Pediatr Neurol. 2015; 52:526–528.
Article6. Ballaban-Gil K, Callahan C, O'Dell C, Pappo M, Moshé S, Shinnar S. Complications of the ketogenic diet. Epilepsia. 1998; 39:744–748.
Article7. Nanjo S, Nishikawa J, Miwa S, Mihara H, Fujinami H, Yoshita H, et al. Immune-mediated protein-losing enteropathy with Down syndrome. Intern Med. 2014; 53:2301–2305.
Article8. Dinari G, Rosenbach Y, Zahavi I, Sivan Y, Nitzan M. Random fecal alpha 1-antitrypsin excretion in children with intestinal disorders. Am J Dis Child. 1984; 138:971–973.
Article9. Wang SJ, Tsai SC, Lan JL. Tc-99m albumin scintigraphy to monitor the effect of treatment in protein-losing gastroenteropathy. Clin Nucl Med. 2000; 25:197–199.
Article10. Braamskamp MJ, Dolman KM, Tabbers MM. Clinical practice. Protein-losing enteropathy in children. Eur J Pediatr. 2010; 169:1179–1185.11. van de Ven AA, Hoytema van Konijnenburg DP, Wensing AM, van Montfrans JM. The role of prolonged viral gastrointestinal infections in the development of immunodeficiency-related enteropathy. Clin Rev Allergy Immunol. 2012; 42:79–91.
Article12. Khan RR, Lawson AD, Minnich LL, Martin K, Nasir A, Emmett MK, et al. Gastrointestinal norovirus infection associated with exacerbation of inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2009; 48:328–333.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Primary Sjogren's Syndrome with Protein-losing Enteropathy
- A case of systemic lupus erythematosus with chylothorax, chronic interstitial cystitis and protein-losing enteropathy
- Treatment of Protein-losing Enteropathy After Fontan Procedure by Conversion to the Total Cavopulmonary Connection with Fenestration
- A Case of Protein-losing Enteropathy in Congestive Heart Failure : Resolution with Prednisolone
- A case of constrictive pericarditis presenting with protein-losing enteropathy
