Ewha Med J.
2018 Jul;41(3):45-52. 10.12771/emj.2018.41.3.45.
Comparison of Clinical Manifestation and Laboratory Findings between Adenoviral Infection with or without Kawasaki Disease
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University College of Medicine, Seoul, Korea. ymhong@ewha.ac.kr
- KMID: 2417941
- DOI: http://doi.org/10.12771/emj.2018.41.3.45
Abstract
OBJECTIVES
Adenovirus infection, which has been known to mimic Kawasaki disease (KD), is one of the most frequent conditions observed during differential diagnosis when considering KD. Accordingly, it is essential to being able to differentiate between these two diseases. Therefore, we performed multiplex reverse transcriptase-polymerase chain reaction and tissue-Doppler echocardiography to distinguish between adenovirus patients and KD patients.
METHODS
A total of 113 adenoviral infection patients (female 48, male 65) diagnosed from January 2010 to June 2016 were evaluated. We divided adenoviral infection patients into two groups: group 1, which consisted of individuals diagnosed with KD according to the KD American Heart Association criteria (n=62, KD with adenovirus infection); and group 2, which comprised individuals only diagnosed with adenovirus infection (n=51). Laboratory data were obtained from each patient including N-terminal pro-brain natriuretic peptide. Echocardiographic measurements were compared between two groups. In addition, reverse transcriptase-polymerase chain reaction was performed using nasopharyngeal secretions to diagnose adenoviral infection.
RESULTS
Conjunctival injection, cervical lymphadenopathy, polymorphous skin rash, abnormalities of the lip or oral mucosa and abnormalities of extremities were significantly higher in group 1 than group 2. Moreover, group 1 had significantly higher C-reactive protein and alanine aminotransferase levels, as well as lower platelet counts and albumin levels than group 2. Coronary artery diameter was significantly greater in group 1 than group 2.
CONCLUSION
In patients with adenoviral infection with unexplained prolonged fever, echocardiography and C-reactive protein can be used to differentiate KD with adenoviral infection from adenoviral infection alone.
Keyword
MeSH Terms
-
Adenoviridae
Adenoviridae Infections
Alanine Transaminase
American Heart Association
C-Reactive Protein
Coronary Vessels
Diagnosis, Differential
Echocardiography
Exanthema
Extremities
Fever
Humans
Lip
Lymphatic Diseases
Male
Mouth Mucosa
Mucocutaneous Lymph Node Syndrome*
Platelet Count
Polymerase Chain Reaction
Alanine Transaminase
C-Reactive Protein
Figure
-
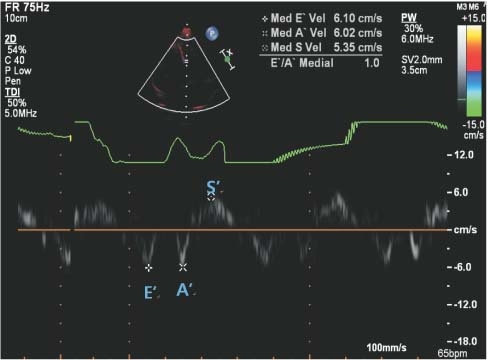
Fig. 1. Myocardial velocity by tissue Doppler imaging in Kawasaki disease patient. E’, early diastolic myocardial velocity; A’, late diastolic myocardial velocity; S’, systolic myocardial velocity.
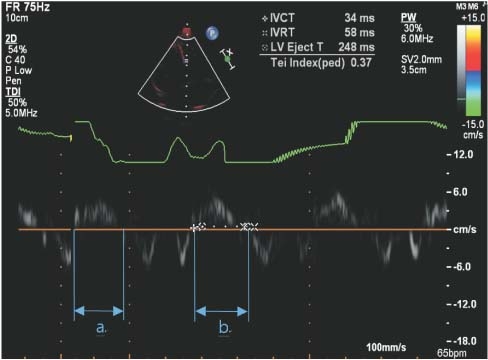
Fig. 2. Tei index by tissue Doppler imaging in Kawasaki disease patient. Tei index=(a-b)/b=(IVCT+IVRT)/LVET. IVCT, isovolumetric contraction time; IVRT, isovolumetric relaxation time; LVET, left ventricle ejection time.
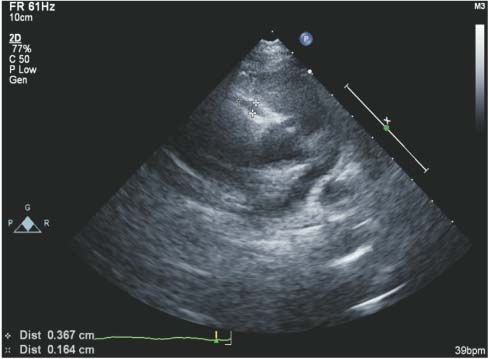
Fig. 3. Right coronary artery dilatation by echocardiography in Kawasaki disease patient.
Reference
-
References
1. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017; 135:e927–e999.
Article2. Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics. 2004; 114:1708–1733.
Article3. Newburger JW, Takahashi M, Burns JC, Beiser AS, Chung KJ, Duffy CE, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med. 1986; 315:341–347.
Article4. Burns JC, Glode MP. Kawasaki syndrome. Lancet. 2004; 364:533–544.
Article5. Jordan-Villegas A, Chang ML, Ramilo O, Mejias A. Concomitant respiratory viral infections in children with Kawasaki disease. Pediatr Infect Dis J. 2010; 29:770–772.
Article6. Rowley AH, Baker SC, Shulman ST, Garcia FL, Fox LM, Kos IM, et al. RNA-containing cytoplasmic inclusion bodies in ciliated bronchial epithelium months to years after acute Kawasaki disease. PLoS One. 2008; 3:e1582.
Article7. Okano M, Thiele GM, Sakiyama Y, Matsumoto S, Purtilo DT. Adenovirus infection in patients with Kawasaki disease. J Med Virol. 1990; 32:53–57.
Article8. Esper F, Shapiro ED, Weibel C, Ferguson D, Landry ML, Kahn JS. Association between a novel human coronavirus and Kawasaki disease. J Infect Dis. 2005; 191:499–502.
Article9. Shike H, Shimizu C, Kanegaye JT, Foley JL, Schnurr DP, Wold LJ, et al. Adenovirus, adeno-associated virus and Kawasaki disease. Pediatr Infect Dis J. 2005; 24:1011–1014.
Article10. Chang LY, Lu CY, Shao PL, Lee PI, Lin MT, Fan TY, et al. Viral infections associated with Kawasaki disease. J Formos Med Assoc. 2014; 113:148–154.
Article11. Song E, Kajon AE, Wang H, Salamon D, Texter K, Ramilo O, et al. Clinical and virologic characteristics may aid distinction of acute adenovirus disease from Kawasaki disease with incidental adenovirus detection. J Pediatr. 2016; 170:325–330.12. Ferone EA, Berezin EN, Durigon GS, Finelli C, Felicio MC, Storni JG, et al. Clinical and epidemiological aspects related to the detection of adenovirus or respiratory syncytial virus in infants hospitalized for acute lower respiratory tract infection. J Pediatr (Rio J). 2014; 90:42–49.
Article13. Rocholl C, Gerber K, Daly J, Pavia AT, Byington CL. Adenoviral infections in children: the impact of rapid diagnosis. Pediatrics. 2004; 113(1 Pt 1):e51–e56.
Article14. Fukuda S, Ito S, Fujiwara M, Abe J, Hanaoka N, Fujimoto T, et al. Simultaneous development of Kawasaki disease following acute human adenovirus infection in monozygotic twins: a case report. Pediatr Rheumatol Online J. 2017; 15:39.
Article15. Turnier JL, Anderson MS, Heizer HR, Jone PN, Glode MP, Dominguez SR. Concurrent respiratory viruses and Kawasaki disease. Pediatrics. 2015; 136:e609–e614.
Article16. Japan Kawasaki Disease Research Committee. Report of subcommittee on standardization of diagnostic criteria and reporting of coronary artery lesions in Kawasaki disease. Tokyo: Ministry of Health and Welfare; 1984.17. Lee SB, Choi HS, Son S, Hong YM. Cardiac function in Kawasaki disease patients with respiratory symptoms. Korean Circ J. 2015; 45:317–324.
Article18. Jaggi P, Kajon AE, Mejias A, Ramilo O, Leber A. Human adenovirus infection in Kawasaki disease: a confounding bystander? Clin Infect Dis. 2013; 56:58–64.
Article19. Kim JH, Yu JJ, Lee J, Kim MN, Ko HK, Choi HS, et al. Detection rate and clinical impact of respiratory viruses in children with Kawasaki disease. Korean J Pediatr. 2012; 55:470–473.
Article20. Heim A, Ebnet C, Harste G, Pring-Akerblom P. Rapid and quantitative detection of human adenovirus DNA by real-time PCR. J Med Virol. 2003; 70:228–239.
Article21. Edwards KM, Thompson J, Paolini J, Wright PF. Adenovirus infections in young children. Pediatrics. 1985; 76:420–424.
Article22. Tabain I, Ljubin-Sternak S, Cepin-Bogovic J, Markovinovic L, Knezovic I, Mlinaric-Galinovic G. Adenovirus respiratory infections in hospitalized children: clinical findings in relation to species and serotypes. Pediatr Infect Dis J. 2012; 31:680–684.23. Colvin JM, Muenzer JT, Jaffe DM, Smason A, Deych E, Shannon WD, et al. Detection of viruses in young children with fever without an apparent source. Pediatrics. 2012; 130:e1455–e1462.
Article24. Barone SR, Pontrelli LR, Krilov LR. The differentiation of classic Kawasaki disease, atypical Kawasaki disease, and acute adenoviral infection: use of clinical features and a rapid direct fluorescent antigen test. Arch Pediatr Adolesc Med. 2000; 154:453–456.25. Kawasaki Y, Hosoya M, Katayose M, Suzuki H. Correlation between serum interleukin 6 and C-reactive protein concentrations in patients with adenoviral respiratory infection. Pediatr Infect Dis J. 2002; 21:370–374.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Characteristics of Lymphadenopathy as the Initial Manifestation of Kawasaki Disease
- Discrimination of Kawasaki disease with concomitant adenoviral detection differentiating from isolated adenoviral infection
- Diagnosis of incomplete Kawasaki disease
- Clinical Analysis and Comparison of Kawasaki Disease between Patients Younger than One Year of Age and Those over One Year of Age
- C-reactive protein and N-terminal pro-brain natriuretic peptide discrepancy: a differentiation of adenoviral pharyngoconjunctival fever from Kawasaki disease
