Apocrine Encapsulated Papillary Carcinoma of the Breast: The First Reported Case with an Infiltrative Component
- Affiliations
-
- 1Department of Pathology, University of Szeged, Szeged, Hungary. kovari.bence.p@gmail.com
- 2Department of Radiology, University of Szeged, Szeged, Hungary.
- 3Affidea Diagnostics-Szeged, Szeged, Hungary.
- 4Department of Surgery, University of Szeged, Szeged, Hungary.
- 5Department of Pathology, Bács-Kiskun County Teaching Hospital, Kecskemét, Hungary.
- KMID: 2413943
- DOI: http://doi.org/10.4048/jbc.2018.21.2.227
Abstract
- Apocrine encapsulated papillary carcinoma (EPC) of the breast is a rare neoplasm, and only 10 cases have been reported in the literature to date. Although EPC by definition lacks a peripheral myoepithelial layer, all previously published apocrine EPC cases were clinically indolent and lacked a conventional invasive component. Herein, we report the 11th case of apocrine EPC, which had a conventional invasive carcinoma component and provides evidence of the malignant potential of this entity. We postulate that apocrine EPC is most likely a morphological variant of conventional EPC, with the same unpredictable malignant potential as non-apocrine cases.
Keyword
Figure
-
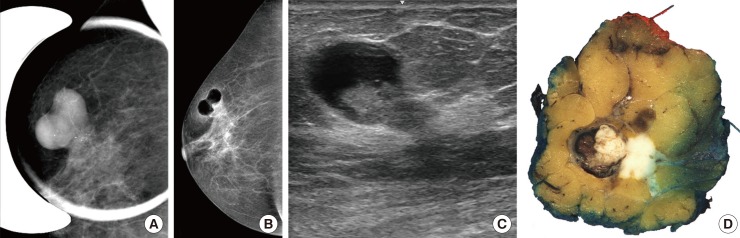
Figure 1 Imaging and gross findings. Architecture of the dual tumor with mammography (A), pneumocystography (B), ultrasound (C), and gross morphology (D). Note the sharply outlined component, showing a clear cystic nature (B, C) with an intraluminal mass. In connection with the intracystic tumor an ill-defined lesion with coarse microcalcifications (A) suggestive of an infiltrative tumor component is also present.
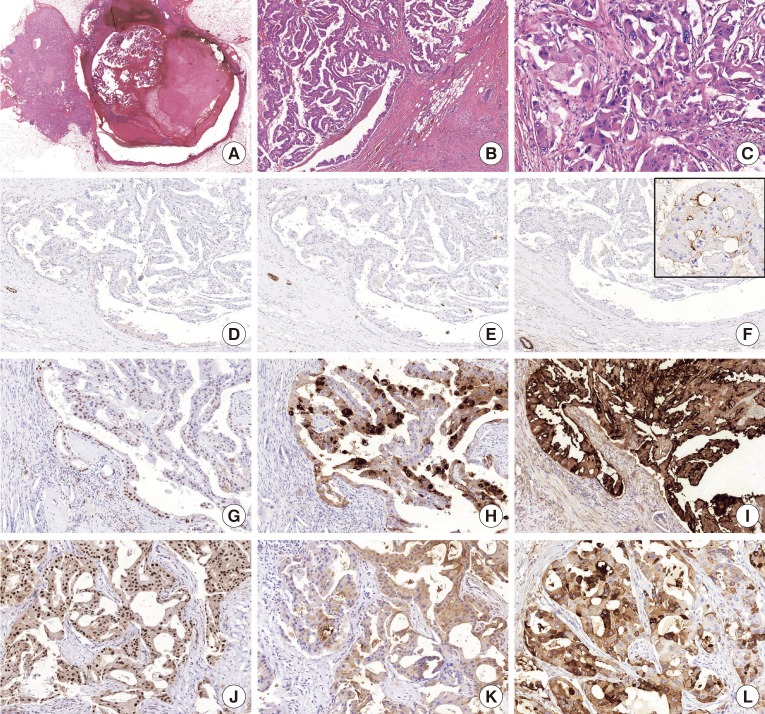
Figure 2 Histological characteristics and immunoprofile. (A) An intracystic papillary component (right) is surrounded by a thick fibrous capsule and an invasive carcinoma (left) component on the low-power view of the lesion (H&E stain, ×1.2). (B) The intracystic part shows a prominent papillary architecture and apocrine cytomorphology (H&E stain, ×5). (C) The invasive carcinoma part also demonstrates apocrine cytomorphology (H&E stain, ×20). The p63 (D, H&E stain, ×5), cytokeratin 5 (E, H&E stain, ×5), and CD10 (F, H&E stain, ×5) immunohistochemistry markers demonstrate the absence of myoepithelial cells in the intracystic papillary component; note the positive internal control and the focal luminal CD10 expression (insert) frequently observed in apocrine lesions [13]. As an evidence for apocrine differentiation, both the encapsulated papillary carcinoma component (G-I, ×15) and the invasive component (J-L, ×20) express androgen receptor (G and J, respectively), gross cystic disease fluid protein 15 (H and K, respectively), and growth hormone-releasing hormone-receptor (I and L, respectively).
Reference
-
1. Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ. WHO Classification of Tumours of the Breast. 4th ed. Lyon: International Agency for Research on Cancer;2012.2. Esposito NN, Dabbs DJ, Bhargava R. Are encapsulated papillary carcinomas of the breast in situ or invasive? A basement membrane study of 27 cases. Am J Clin Pathol. 2009; 131:228–242. PMID: 19141383.3. Rakha EA, Ahmed MA, Ellis IO. Papillary carcinoma of the breast: diagnostic agreement and management implications. Histopathology. 2016; 69:862–870. PMID: 27270947.
Article4. Tan PH, Schnitt SJ, van de Vijver MJ, Ellis IO, Lakhani SR. Papillary and neuroendocrine breast lesions: the WHO stance. Histopathology. 2015; 66:761–770. PMID: 24845113.
Article5. Leal C, Costa I, Fonseca D, Lopes P, Bento MJ, Lopes C. Intracystic (encysted) papillary carcinoma of the breast: a clinical, pathological, and immunohistochemical study. Hum Pathol. 1998; 29:1097–1104. PMID: 9781648.
Article6. Vranic S, Schmitt F, Sapino A, Costa JL, Reddy S, Castro M, et al. Apocrine carcinoma of the breast: a comprehensive review. Histol Histopathol. 2013; 28:1393–1409. PMID: 23771415.7. Kővári B, Rusz O, Schally AV, Kahán Z, Cserni G. Differential immunostaining of various types of breast carcinomas for growth hormonereleasing hormone receptor: apocrine epithelium and carcinomas emerging as uniformly positive. APMIS. 2014; 122:824–831. PMID: 24479854.8. Kővári B, Vranic S, Marchio C, Sapino A, Cserni G. The expression of GHRH and its receptors in breast carcinomas with apocrine differentiation-further evidence of the presence of a GHRH pathway in these tumors. Hum Pathol. 2017; 64:164–170. PMID: 28438614.
Article9. Seal M, Wilson C, Naus GJ, Chia S, Bainbridge TC, Hayes MM. Encapsulated apocrine papillary carcinoma of the breast: a tumour of uncertain malignant potential: report of five cases. Virchows Arch. 2009; 455:477–483. PMID: 19862552.10. Laforga JB, Gasent JM, Sánchez I. Encapsulated apocrine papillary carcinoma of the breast: case report with clinicopathologic and immunohistochemical study. Diagn Cytopathol. 2011; 39:288–293. PMID: 20734358.
Article11. Hayashi H, Ohtani H, Yamaguchi J, Shimokawa I. A case of intracystic apocrine papillary tumor: diagnostic pitfalls for malignancy. Pathol Res Pract. 2013; 209:808–811. PMID: 24095109.
Article12. Kuroda N, Fujishima N, Hayes MM, Moritani S, Ichihara S. Encapsulated papillary carcinoma, apocrine type, of the breast. Malays J Pathol. 2014; 36:139–143. PMID: 25194537.13. Kővári B, Báthori Á, Cserni G. CD10 immunohistochemical expression in apocrine lesions of the breast. Pathobiology. 2015; 82:259–263. PMID: 26562027.
Article14. Cserni G. Lack of myoepithelium in apocrine glands of the breast does not necessarily imply malignancy. Histopathology. 2008; 52:253–255. PMID: 18184276.
Article15. Cserni G. Benign apocrine papillary lesions of the breast lacking or virtually lacking myoepithelial cells: potential pitfalls in diagnosing malignancy. APMIS. 2012; 120:249–252. PMID: 22339683.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Synchronous Encapsulated Papillary Carcinoma and Invasive Ductal Carcinoma Arising from Intraductal Papilloma in the Same Breast: A Case Report
- Apocrine Gland Carcinoma
- Apocrine Carcinoma of the Breast: The report of 2 cases
- Papillary Apocrine Metaplasia of the Breast Mimicking Papillary Neoplasm: A Case Report
- Apocrine Ductal Carcinoma In Situ of the Breast Presented Mass with Morphological Change on Follow-Up Ultrasound: A Report of Case
