Synchronous Encapsulated Papillary Carcinoma and Invasive Ductal Carcinoma Arising from Intraductal Papilloma in the Same Breast: A Case Report
- Affiliations
-
- 1Department of Radiology, Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. taloo@hanmail.net
- 2Department of Pathology, Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea.
- 3Department of Nuclear Medicine, Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea.
- 4Department of Surgery, Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea.
- KMID: 1736480
- DOI: http://doi.org/10.3348/jksr.2014.71.3.139
Abstract
- Encapsulated papillary carcinoma of the breast is rare, accounting for just 0.5% to 2% of all breast cancers. A histological upgrade from papillary lesion can also possibly occur, however, an upgrade to invasive ductal carcinoma has uncommonly been reported. Furthermore, to the best of our knowledge, there is no reported case of encapsulated papillary carcinoma and invasive ductal carcinoma arising from intraductal papilloma in the same breast. We report an extremely rare case of synchronous encapsulated papillary carcinoma and invasive ductal carcinoma arising from intraductal papilloma on the same breast with radiologic-pathologic correlation.
Figure
-
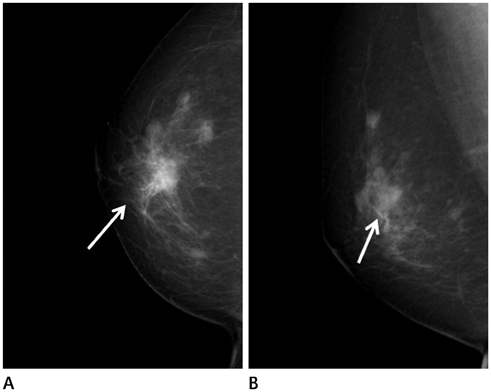
Fig. 1 A 56-year-old woman with outside biopsy proven invasive ductal carcinoma. Right craniocaudal (A) and mediolateral oblique mammography (B) show about 1.5 cm sized partly indistinct oval hyperdense mass in right breast upper center, which is biopsy proven malignancy (arrow). There are several circumscribed oval isodense nodules around this lesion.
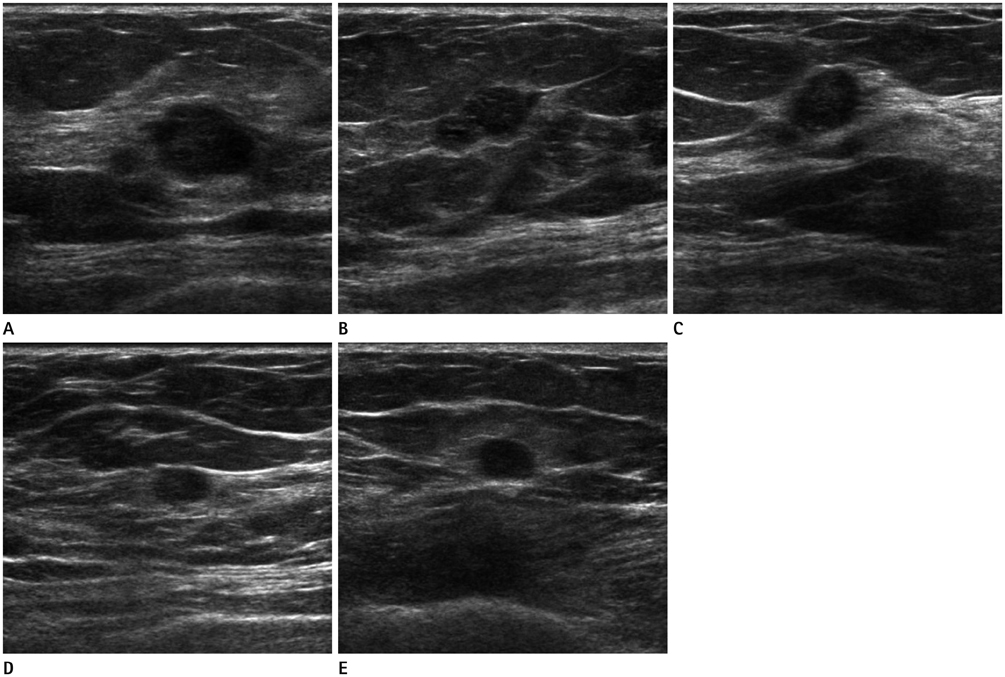
Fig. 2 Ultrasonography shows a 1.2 cm sized partly angular oval hypoechoic mass, which is biopsy proven malignancy (A) and a 1.3 cm sized microlobulated oval hypoechoic mass (B) in right breast upper center. A partly angular round hypoechoic mass (C), circumscribed oval hypoechoic mass (D) in right breast upper outer and a circumscribed oval hypoechoic mass (E) in right breast upper inner are also noted.

Fig. 3 The axial dynamic-enhanced T1-weighted image of the first post-contrast acquisition shows rim enhancement for masses in right breast upper center, outer (A, B) and inner (C, arrow).

Fig. 4 Enhancement patterns of masses in right breast. A, B. The kinetic curve shows early enhancement and a plateau pattern for biopsy proven malignancy (A) and a enhancing mass (B) in right breast upper inner (same as above in others, not shown).
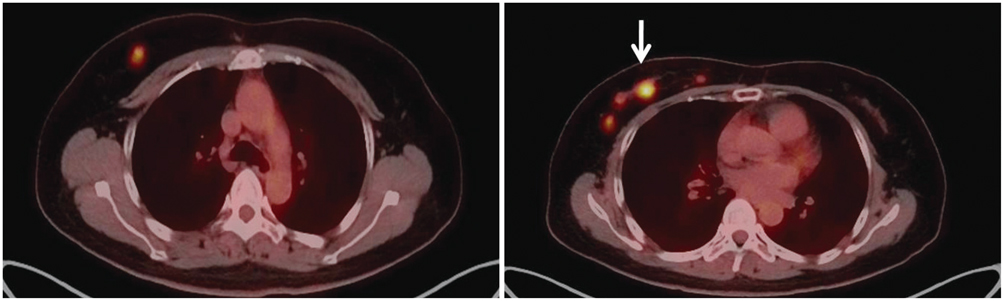
Fig. 5 On the axial positron emission tomography/CT fusion image, the biopsy proven malignancy shows hypermetabolism with a peak standardized uptake value of 10.21 (arrow) and other nodules also show increased fluorodeoxyglucose uptake.

Fig. 6 Microscopic findings of pathologic confirmed invasive ductal carcinomas arising in intraductal papilloma. A-C. Invasive ductal carcinoma arising in intraductal papilloma (biopsy proven malignancy, corresponding with Fig. 2A). Multiple papillae in complex arborizing pattern (× 12.5) (A). Nests or cords infiltrate adjacent stroma showing invasion (× 100) (arrow) (B). Well-developed papillary architecture is found (× 100) (arrow) (C). D-F. Invasive ductal carcinoma arising in intraductal papilloma (upper center, Fig. 2B). Microphotograph showing a well-circumscribed mass containing well-developed papillary architecture (× 12.5) (D). Nests or cords infiltrate adjacent stroma showing invasion (× 100) (arrow) (E). Well-developed papillary architecture is found (× 100) (arrow) (F). G-I. Invasive ductal carcinoma arising in intraductal papilloma (upper outer, Fig. 2C). Microphotograph showing a well-circumscribed mass containing well-developed papillary or cribriform architecture. Glandular proliferation within stalks may resemble cribriform architecture (× 12.5) (G). Nests or cords infiltrate adjacent stroma showing invasion (× 100) (arrow) (H). Well-developed cribriform architecture is found (× 100) (arrow) (I). J-L. Invasive ductal carcinoma arising in intraductal papilloma (far upper outer, Fig. 2D). Microphotograph showing a well-circumscribed mass containing well-developed papillary architecture (× 12.5) (J). Nests or cords infiltrate adjacent stroma showing invasion (× 100) (arrow) (K). Well-developed papillary or cribriform architecture are found (× 100) (arrow) (L).

Fig. 7 Microscopic findings of pathologic confirmed encapsulated papillary carcinoma. A. Encapsulated papillary carcinoma has thick fibrous capsule (yellow arrow) and adjacent low grade ductal carcinoma in situ (blue arrow). Red arrow indicates artifact, not true invasion (probably rupture during surgery procedure), because there is no stromal reaction (× 12.5). B, C. Well-developed papillae with cytologic atypia are found (× 40). D-F. Immunohistochemical staining is negative for SMM-HC, p63, and CK 5/6, showing absence of myoepithelial cells (× 40).
Reference
-
1. Mercado CL, Hamele-Bena D, Oken SM, Singer CI, Cangiarella J. Papillary lesions of the breast at percutaneous core-needle biopsy. Radiology. 2006; 238:801–808.2. Liberman L, Tornos C, Huzjan R, Bartella L, Morris EA, Dershaw DD. Is surgical excision warranted after benign, concordant diagnosis of papilloma at percutaneous breast biopsy? AJR Am J Roentgenol. 2006; 186:1328–1334.3. Chang JM, Moon WK, Cho N, Han W, Noh DY, Park IA, et al. Risk of carcinoma after subsequent excision of benign papilloma initially diagnosed with an ultrasound (US)-guided 14-gauge core needle biopsy: a prospective observational study. Eur Radiol. 2010; 20:1093–1100.4. Esposito NN, Dabbs DJ, Bhargava R. Are encapsulated papillary carcinomas of the breast in situ or invasive? A basement membrane study of 27 cases. Am J Clin Pathol. 2009; 131:228–224.5. Liberman L. Clinical management issues in percutaneous core breast biopsy. Radiol Clin North Am. 2000; 38:791–807.6. MacGrogan G, Tavassoli FA. Central atypical papillomas of the breast: a clinicopathological study of 119 cases. Virchows Arch. 2003; 443:609–617.7. Rosen PP. Rosen's breast pathology. Philadelphia, PA: Lippincott-Raven;1997. p. 335–354.8. Carter D, Orr SL, Merino MJ. Intracystic papillary carcinoma of the breast. After mastectomy, radiotherapy or excisional biopsy alone. Cancer. 1983; 52:14–11.9. Soo MS, Williford ME, Walsh R, Bentley RC, Kornguth PJ. Papillary carcinoma of the breast: imaging findings. AJR Am J Roentgenol. 1995; 164:321–326.10. Bhatia A, Nahar Saikia Uma, Kumar Y. Rare coexistence of invasive papillary carcinoma with infiltrating ductal carcinoma in male breast: report of a case. Int J Surg Pathol. 2008; 16:311–313.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Lobular Carcinoma of the Breast Associated with Mixed Lobular and Ductal Carcinoma In Situ: A Case Report
- The Galectin 3 Expression in Benign and Malignant Breast Tumor
- Invasive Ductal Carcinoma Arising within a Mammary Hamartoma: Case Report
- A Case of Central Nervous System Toxicity Assoclated with Cyclosporine
- Invasive Micropapillary Carcinoma in Axillary Ectopic Breast and Synchronous Ductal Carcinoma In Situ in the Contralateral Breast
