C2 Segmental-Type Vertebral Artery Diagnosed Using Computed Tomographic Angiography
- Affiliations
-
- 1Department of Neurosurgery, National Medical Center, Seoul, Korea. hanibalkms@hanmail.net
- KMID: 2408020
- DOI: http://doi.org/10.3340/jkns.2017.0303.010
Abstract
OBJECTIVE
Sometimes a vertebral artery (VA) enters the spinal canal via the C1-2 intervertebral space, a variation regarded as a C2 segmental-type VA. This paper describes the anatomy of the C2 segmental-type VA and reviews its clinical importance.
METHODS
Between March 2014 and November 2015, 3386 patients underwent computed tomographic angiography. I identified C2 segmental-type VAs, associated vascular variation, the origin of ipsilateral posterior inferior cerebellar arteries (PICAs), and the clinical symptoms associated with C2 segmental-type VAs. The origin of an ipsilateral PICA is divided into 5 types. A type 1 PICA originates from ipsilateral VAs coursing suboccipitally (IVASO), a type 2 originates from ipsilateral proximal C2 segmental-type VAs, a type 3 originates from ipsilateral distal C2 segmental-type VAs. For type 4, the PICA does not originate from an ipsilateral VA. For type 5, the PICA is the terminal end of an ipsilateral C2 segmental-type VA.
RESULTS
One hundred thirteen patients had 121 C2 segmental-type VAs; 47 were associated with an IVASO, and 74 were not. Four type 1, 13 type 2, 60 type 3, 42 type 4, and two type 5 PICAs were identified. Only one patient showed symptoms associated with a C2 segmental-type VA, being a 71-year-old man presenting with a C2 segmental-type VA infarction.
CONCLUSION
For C2 segmental-type VAs, the ipsilateral IVASO and origin of the PICA are important for predicting the outcome of this type of VA infarction.
MeSH Terms
Figure
-

Fig. 1 Origins of the ipsilateral posterior inferior cerebellar artery (PICA) from the C2 segmental-type vertebral artery (VA). The type 1 PICA originates from the ipsilateral VA, coursing suboccipitally (ipsilateral VAs coursing suboccipitally, blue segment). The type 2 PICA originates from the ipsilateral proximal C2 segmental-type VA (white segment). The type 3 PICA originates from the ipsilateral distal VA (red segment). The type 4 PICA does not originate from the VA between the C2 vertebral foramen and the vertebrobasilar junction. In type 5, the PICA is the terminal end of the ipsilateral C2 segmental-type VA. The left PICA (red arrowhead) is type 2.

Fig. 2 Computed tomographic angiography of a 61-year-old man showing a left C2 segmental-type vertebral artery (VA, red arrow) with ipsilateral VA coursing suboccipitally (ipsilateral VAs coursing suboccipitally [IVASO], red arrowhead) (A). Coronal computed tomography showing the left C2 segmental-type VA (black arrow) entering the spinal canal between the C1 and C2 vertebrae and the IVASO (black arrowhead) entering the spinal canal between the atlas and occiput (B).

Fig. 3 Computed tomographic angiography of a 64-year-old man showing a left C2 segmental-type vertebral artery (red arrow, A). Coronal computed tomography showing the left vertebral artery entering the spinal canal between C1 and C2 (black arrow, B).
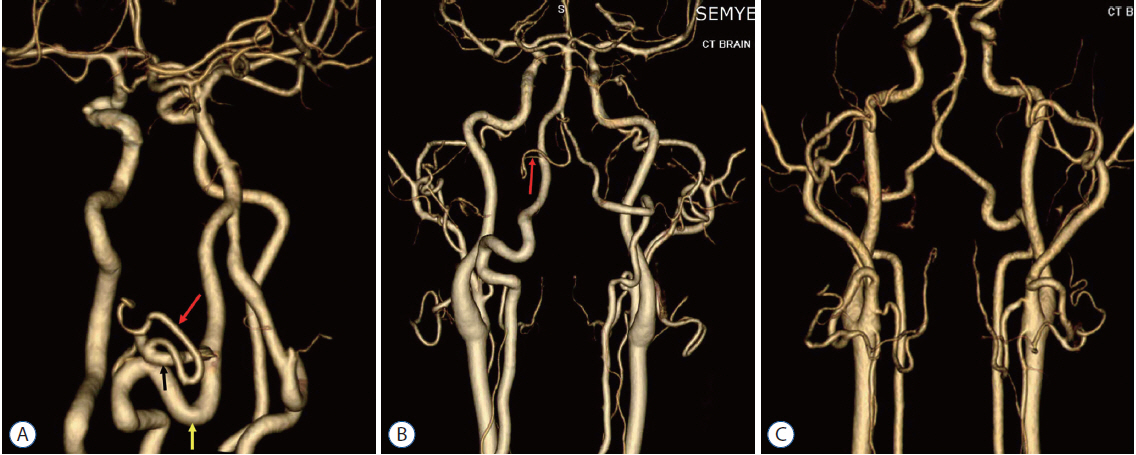
Fig. 4 Types of posterior inferior cerebellar arteries (PICAs) originating from a vertebral artery (VA). Type 1 (red arrow) originating from an ipsilateral VA coursing suboccipitally (black arrow; C2 segmental-type VA, yellow arrow) (A). Type 3 (red arrow) originating from a distal C2 segmental-type VA (B). C2 segmental-type vertebral artery with no PICA branch (type 4, C).
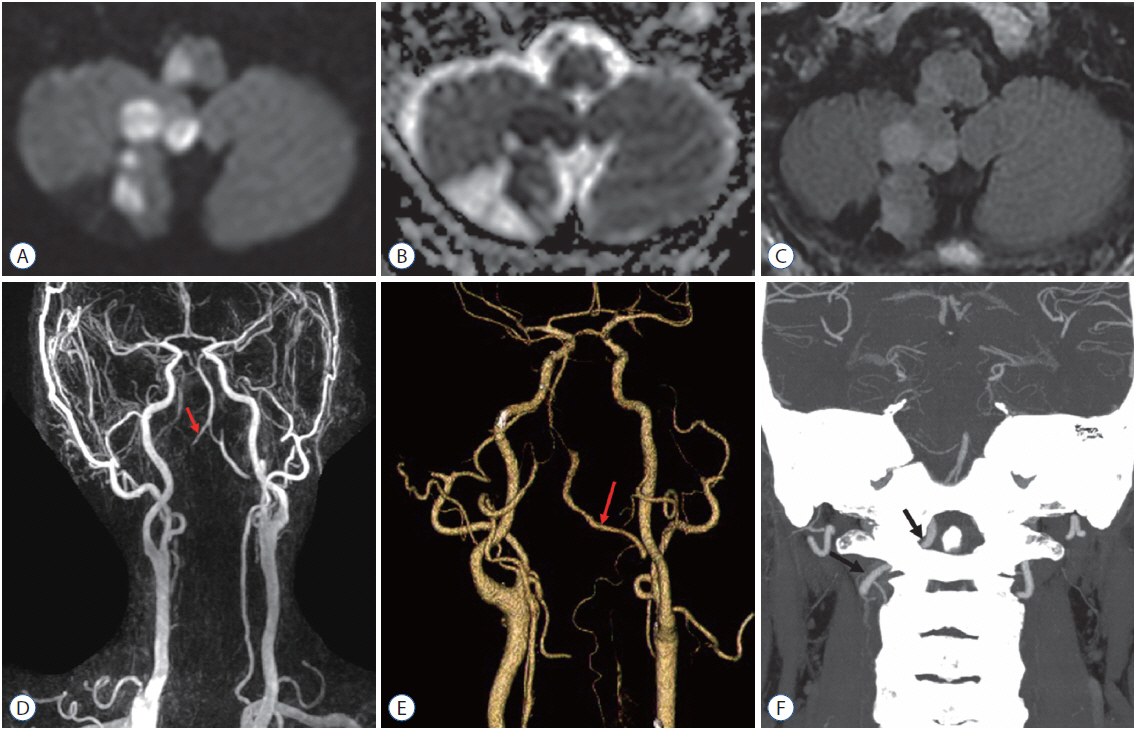
Fig. 5 Brain magnetic resonance images (A : diffusion-weighted image, B : apparent diffusion coefficient map, C : fluid-attenuated inversion-recovery image) showing an old right cerebellar infarction and a recent infarction involving the right cerebellum and right lateral medulla. Magnetic resonance angiography (D) demonstrating no sign of the right vertebral artery except for a terminal segment (red arrow). Computed tomographic angiography (E) performed 6 months later demonstrating a partially recanalized right C2 segmental-type vertebral artery (red arrow). Coronal computed tomography (F) showing a right C2 segmental-type vertebral artery (black arrow).
Reference
-
References
1. Bernard TJ, Mull BR, Handler MH, Harned RK, Filley CM, Kumpe DA, et al. An 18-year-old man with fenestrated vertebral arteries, recurrent stroke and successful angiographic coiling. J Neurol Sci. 260:279–282. 2007.
Article2. Chen CJ, Wang LJ, Wong YC. Abnormal origin of the vertebral artery from the common carotid artery. Am J Neuroradiol. 19:1414–1416. 1998.3. Furumoto T, Nagase J, Takahashi K, Itabashi T, Iai H, Ishige N. Cervical myelopathy caused by the anomalous vertebral artery. A case report. Spine (Phila Pa 1976). 21:2280–2283. 1996.4. Hasegawa T, Kubota T, Ito H, Yamamoto S. Symptomatic duplication of the vertebral artery. Surg Neurol. 20:244–248. 1983.
Article5. Hayashi T, Hirose Y, Sagoh M, Murakami H. Spontaneous occlusion of ruptured vertebral artery dissection at the extradural fenestration associated with extradural origin of the posterior inferior cerebellar artery--case report. Neurol Med Chir (Tokyo). 40:164–168. 2000.
Article6. Kim K, Mizunari T, Kobayashi S, Ishii S, Teramoto A. Occipital neuralgia caused by the compression of the fenestrated vertebral artery: a case report. No Shinkei Geka. 27:645–650. 1999.7. Kim MS. Developmental anomalies of the distal vertebral artery and posterior inferior cerebellar artery: diagnosis by CT angiography and literature review. Surg Radiol Anat. 38:997–1006. 2016.
Article8. Lasjaunias P, Berenstein A, ter Brugge KG. Arterial supply to the posterior fossa central nervous system. In : Lasjaunias P, Berenstein A, ter Brugge KG, editors. Surgical Neuroangiography, Clinical vascular anatomy and variaions. ed 2. New York: Springer Verlag Berlin Heidelberg;2001. 1:p. 224–260.9. Lasjaunias P, Vallee B, Person H, Ter Brugge K, Chiu M. The lateral spinal artery of the upper cervical spinal cord. Anatomy, normal variations, and angiographic aspects. J Neurosurg. 63:235–241. 1985.10. Mayer PL, Kier EL. The ontogeneti and phylogenetic basis of cerebrovascular anomalies and variants. In : Apuzzo MLJ, editor. Brain surgery, complication avoidance and management. New York: Churchill Livingstone;1993. 1:p. 709–760.11. Siclari F, Burger IM, Fasel JH, Gailloud P. Developmental anatomy of the distal vertebral artery in relationship to variants of the posterior and lateral spinal arterial systems. Am J Neuroradiol. 28:1185–1190. 2007.
Article12. Takahashi Y, Sugita S, Uchikado H, Miyagi T, Tokutomi T, Shigemori M. Cervical myelopathy due to compression by bilateral vertebral arteries--case report. Neurol Med Chir (Tokyo). 41:322–324. 2001.
Article13. Takahashi T, Tominaga T, Hassan T, Yoshimoto T. Cervical cord compression with myelopathy caused by bilateral persistence of the first intersegmental arteries: case report. Neurosurgery. 53:234–237. 2003.
Article14. Takei H, Sagae M, Chiba K, Ogino T. The long-term follow-up of surgical treatment for cervical myelopathy with severe nape and upper arm pain caused by the anomalous vertebral artery: case report. Spine (Phila Pa 1976). 33:E611–E613. 2008.15. Tokuda K, Miyasaka K, Abe H, Abe S, Takei H, Sugimoto S, et al. Anomalous atlantoaxial portions of vertebral and posterior inferior cerebellar arteries. Neuroradiology. 27:410–413. 1985.
Article16. Tran-Dinh HD, Soo YS, Jayasinghe LS. Duplication of the vertebro-basilar system. Australas Radiol. 35:220–224. 1991.
Article17. Trimble C, Reeves A, Pare L, Tsai F. Vertebral artery anomaly causing C2 suboccipital neuralgia, relieved by neurovascular decompression. J Neuroimaging. 23:421–424. 2013.
Article18. Uchino A, Saito N, Uemiya N, Sonada KI. Diagnosis of a C3 segmental type of vertebral artery by magnetic resonance angiography: report of two cases. Surg Radiol Anat. 38:873–876. 2016.
Article19. Yoshida T, Shiga K, Uraoka M, Yoshikawa K, Owada K, Nakagawa M. C2 segmental type of vertebral artery with recurrent embolic strokes. Cerebrovasc Dis. 20:58–61. 2005.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk of Vertebral Artery Injury: A Comparison between C2 Subarticular Segmental and C1-2 Transarticular Screws
- A Type 1 Persistent Proatlantal Artery Originating from the External Carotid Artery Detected by Computed Tomographic Angiography
- Vertebral Artery Dissection Presenting with Acute Infarction in Cervical Spinal Cord and Cerebellum
- Rotational vertebral artery syndrome treated via an anterior approach and selective decompression only
- Atlantoaxial Fixation using C2 Subarticular Screws and C1 Lateral Mass Screws : A Technical Report
