Rotational vertebral artery syndrome treated via an anterior approach and selective decompression only
- Affiliations
-
- 1Depertment of Neurosurgery, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Republic of Korea. isbrzw@gmail.com
- KMID: 2465246
- DOI: http://doi.org/10.7461/jcen.2019.21.3.158
Abstract
- We present the case of a 38-year-old male who complained of repeated dizziness and syncope. Rotational vertebral artery syndrome (RVAS) was diagnosed via videonystagmoraphy (VNG), computed tomography angiography (CTA) and three-position digital subtraction angiography (DSA). In the neutral position, CTA and DSA revealed left vertebral artery (VA) stenosis at the C2 transverse foramen and right VA hypoplasia. When the head was turned to the right, the blood flow stopped at the C2 level. The bony structure around the VA at the C2 transverse foramen was decompressed via an anterior surgical approach, and the symptoms resolved. This case present the precise stenotic point evaluation by three-position DSA is crucial for the planning of surgical treatment.
Keyword
MeSH Terms
Figure
-
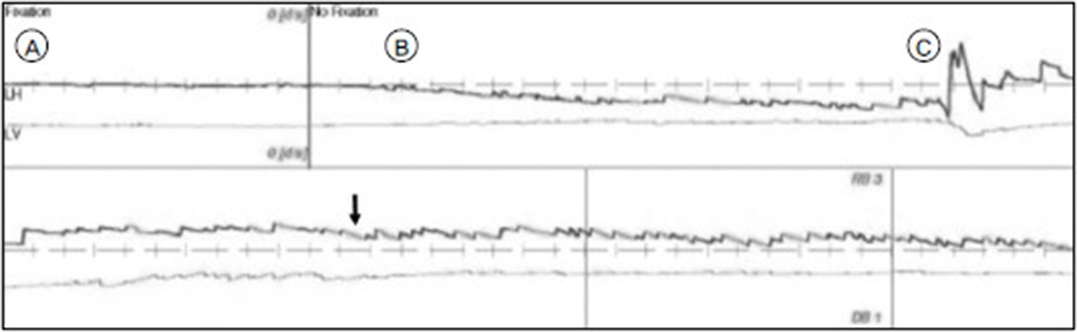
Fig. 1 Videonystagmography revealed no nystagmus in the neutral position (A) or when the head was turned to the left (B). Right-beating nystagmus (black arrow) with a down-beat component was observed when the head was turned to the right (C).
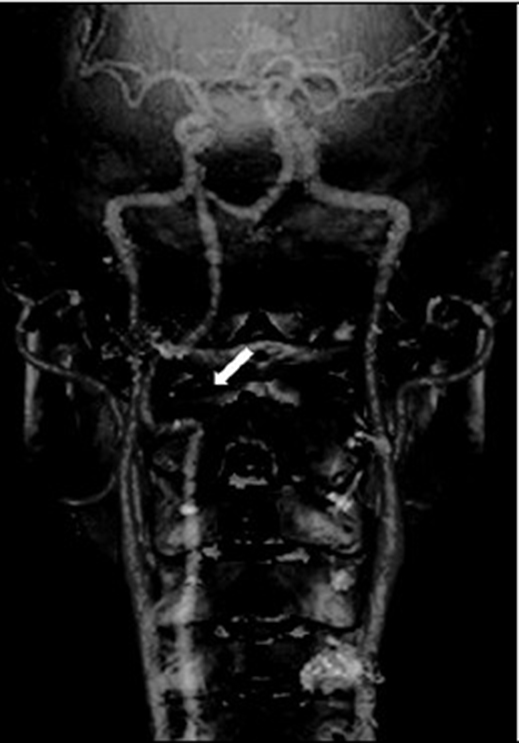
Fig. 2 The posteroanterior view of three-dimensional-reconstruction computed tomography angiography revealed left vertebral artery stenosis at the C2 transverse foramen (white arrow).
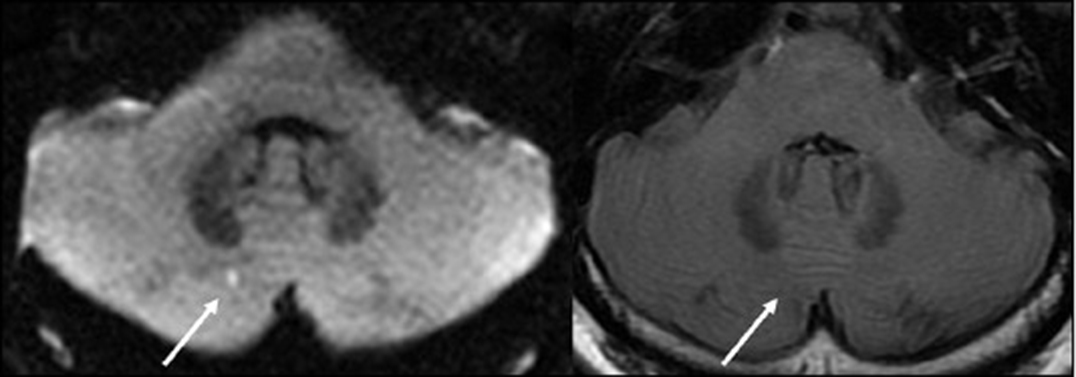
Fig. 3 Diffusion and T2 FLAIR magnetic resonance imaging shows a tiny acute ischemic infarction in the right cerebellum (right arrow).
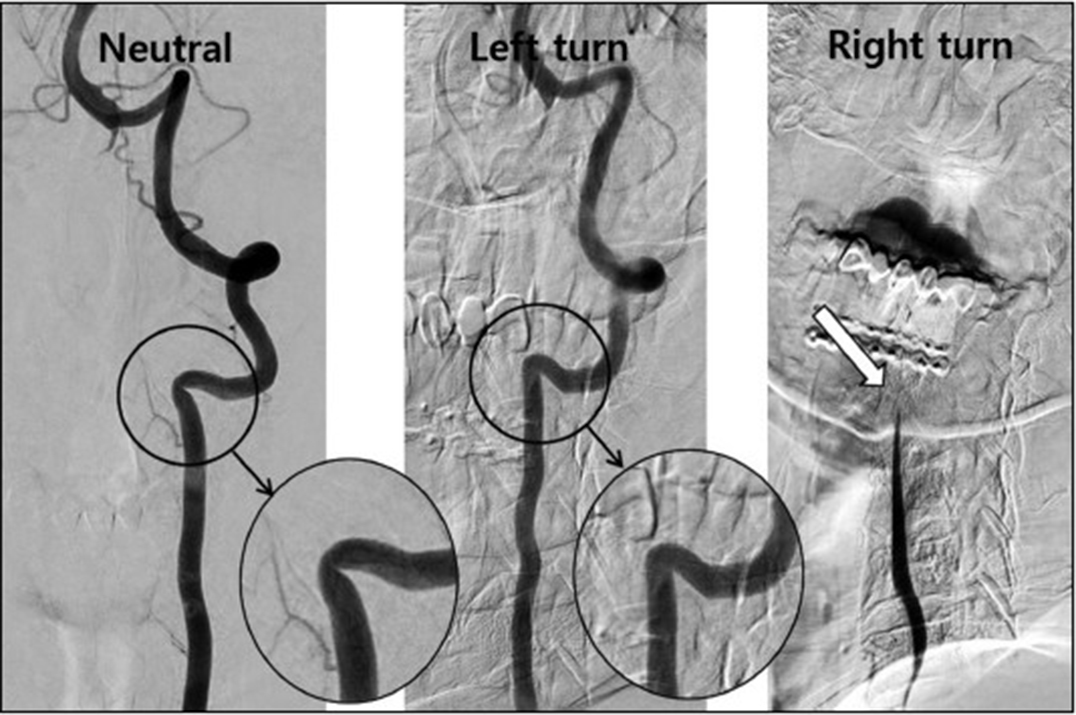
Fig. 4 Neutral. The anteroposterior view of left vertebral artery (VA) angiography with the head in the neutral position revealed left VA stenosis at the C2 transverse foramen. Left turn. The lateral view of left VA angiography when the head was turned to the left revealed that the stenotic VA at C2 became wider than in the neutral position. Right turn. The lateral view of left VA angiography when the head was turned to the right showed that blood flow decreased at the C3–4 level (black arrow) and stopped at the C2 level (white arrow).

Fig. 5 A) Preoperative computed tomography (CT) three-dimensional (3D)-reconstruction image. B) The postoperative CT 3D-reconstruction image showed that the anterior portion of the transverse foramen had been removed; the foramen was thus widened while preserving the articular facet (black arrow).
Reference
-
1. Mekki S. The role of videonystagmography (VNG) in assessment of dizzy patient. Egypt J Otolaryngol. 2014; 30(2):69–72. DOI: 10.4103/1012-5574.133167.
Article2. Choi KD, Choi JH, Kim JS, Kim HJ, Kim MJ, Lee TH, et al. Rotational vertebral artery occlusion: mechanisms and long-term outcome. Stroke. 2013; 44(7):1817–1824. DOI: 10.1161/STROKEAHA.113.001219. PubMed PMID: 23696552.
Article3. Duan G, Xu J, Shi J, Cao Y. Advances in the Pathogenesis, Diagnosis and Treatment of Bow Hunter's Syndrome: A Comprehensive Review of the Literature. Interv Neurol. 2016; 5(1-2):29–38. DOI: 10.1159/000444306. PubMed PMID: 27610119; PubMed Central PMCID: PMCPMC4934473.
Article4. Lu DC, Zador Z, Mummaneni PV, Lawton MT. Rotational vertebral artery occlusion-series of 9 cases. Neurosurgery. 2010; 67(4):1066–1072. DOI: 10.1227/NEU.0b013e3181ee36db. discussion 72. PubMed PMID: 20881570.
Article5. Zaidi HA, Albuquerque FC, Chowdhry SA, Zabramski JM, Ducruet AF, Spetzler RF. Diagnosis and management of bow hunter's syndrome: 15-year experience at barrow neurological institute. World Neurosurg. 2014; 82(5):733–738. DOI: 10.1016/j.wneu.2014.02.027. PubMed PMID: 24549025.6. Matsuyama T, Morimoto T, Sakaki T. Comparison of C1-2 posterior fusion and decompression of the vertebral artery in the treatment of bow hunter's stroke. J Neurosurg. 1997; 86(4):619–623. DOI: 10.3171/jns.1997.86.4.0619. PubMed PMID: 9120624.
Article7. Büttner U, Helmchen C, Brandt T. Diagnostic Criteria for Central versus Peripheral Positioning Nystagmus and Vertigo: a Review. Acta Otolaryngol. 1999; 119(1):1–5. DOI: 10.1080/00016489950181855.8. Wakayama K, Murakami M, Suzuki M, Ono S, Shimizu N. Ischemic symptoms induced by occlusion of the unilateral vertebral artery with head rotation together with contralateral vertebral artery dissection--case report. J Neurol Sci. 2005; 236(1-2):87–90. DOI: 10.1016/j.jns.2005.04.010. PubMed PMID: 15979646.
Article9. Jost GF, Dailey AT. Bow hunter's syndrome revisited: 2 new cases and literature review of 124 cases. Neurosurg Focus. 2015; 38(4):E7. DOI: 10.3171/2015.1.FOCUS14791. PubMed PMID: 25828501.
Article10. Toole JF, Tucker SH. Influence of head position upon cerebral circulation: studies on blood flow in cadavers. Arch Neurol. 1960; 2(6):616–623.11. Seki T, Hida K, Akino M, Iwasaki Y. Anterior decompression of the atlantoaxial vertebral artery to treat bow hunter's stroke: technical case report. Neurosurgery. 2001; 49(6):1474–1476. Epub 2002/02/28. PubMed PMID: 11859829.
Article12. Cevik S, Katar S, Hanımoǧlu H. C1–C2 transverse foramen decompression by anterolateral approach as an alternative treatment in Bow Hunter's Syndrome. Asian J Neurosurg. 2018; 13(2):411.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rotational Vertebral Artery Compression : Bow Hunter's Syndrome
- A Case of Rotational Vertebral Artery Syndrome Treated by Posterior Cervical Decompression
- Cervicogenic Vertigo Treated by C1 Transverse Foramen Decompression : A Case Report
- Iatrogenic Vertebral Artery Injury During Anterior Cervical Spine Surgery : Report of Two Cases
- Rotational Vertebral Artery Syndrome (Bow Hunter’s Syndrome): A Rare Differential Diagnosis in Patients With Syncope
