Acromegaly with Normal Insulin-Like Growth Factor-1 Levels and Congestive Heart Failure as the First Clinical Manifestation
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea. jik1016@dreamwiz.com
- 2Department of Cardiology, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
- KMID: 2407092
- DOI: http://doi.org/10.3803/EnM.2015.30.3.395
Abstract
- The leading cause of morbidity and mortality in patients with acromegaly is cardiovascular complications. Myocardial exposure to excessive growth hormone can cause ventricular hypertrophy, hypertension, arrhythmia, and diastolic dysfunction. However, congestive heart failure as a result of systolic dysfunction is observed only rarely in patients with acromegaly. Most cases of acromegaly exhibit high levels of serum insulin-like growth factor-1 (IGF-1). Acromegaly with normal IGF-1 levels is rare and difficult to diagnose. Here, we report a rare case of an acromegalic patient whose first clinical manifestation was severe congestive heart failure, despite normal IGF-1 levels. We diagnosed acromegaly using a glucose-loading growth hormone suppression test. Cardiac function and myocardial hypertrophy improved 6 months after transsphenoidal resection of a pituitary adenoma.
MeSH Terms
Figure
-
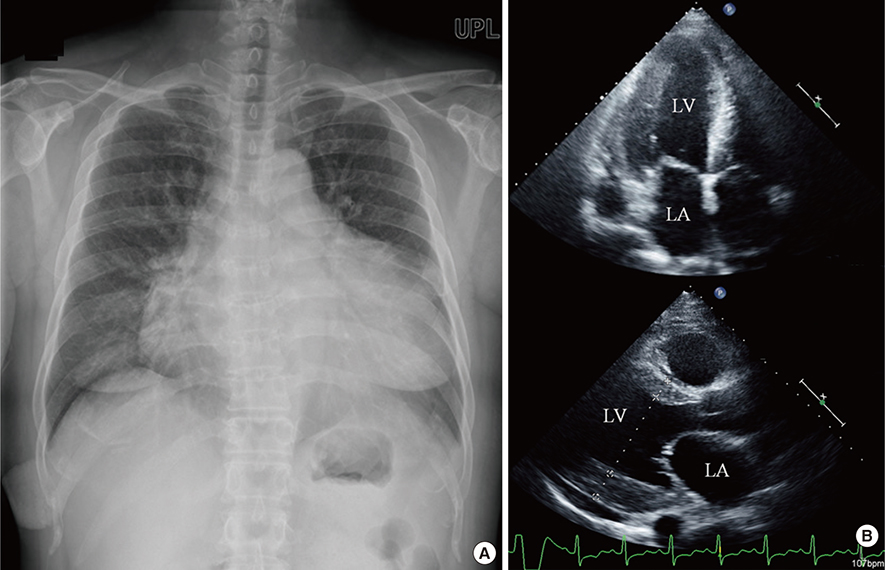
Fig. 1 Chest X-ray and echocardiogram findings showed marked cardiomegaly and left ventricle (LV) hypertrophy. (A) Marked cardiomegaly was detected on chest X-ray. (B) Echocardiogram showed an enlarged left atrium (LA) and LV with concentric LV hypertrophy.

Fig. 2 Clinical manifestations and radiographic findings showed the distinguishing features of acromegaly. (A) Jaw enlargement and frontal bone protrusion. (B) Soft tissue overgrowth of the hand (black arrow) compared with a normal adult hand (white arrow). (C) Soft tissue overgrowth of the heel pad in a foot X-ray.

Fig. 3 Magnetic resonance imaging of the sella showed a suspicious 5-mm linear shape delayed enhancing lesion at the midline to the left side of the pituitary gland (arrow).
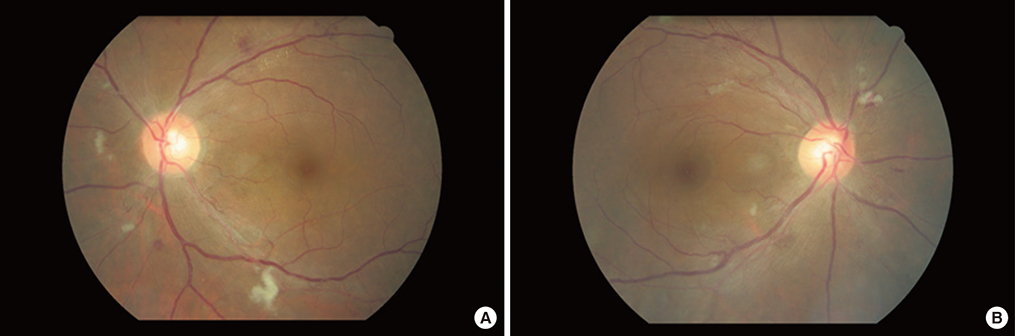
Fig. 4 (A, B) Fundoscopic findings showed cotton wool patches and hemorrhage on both retinae.
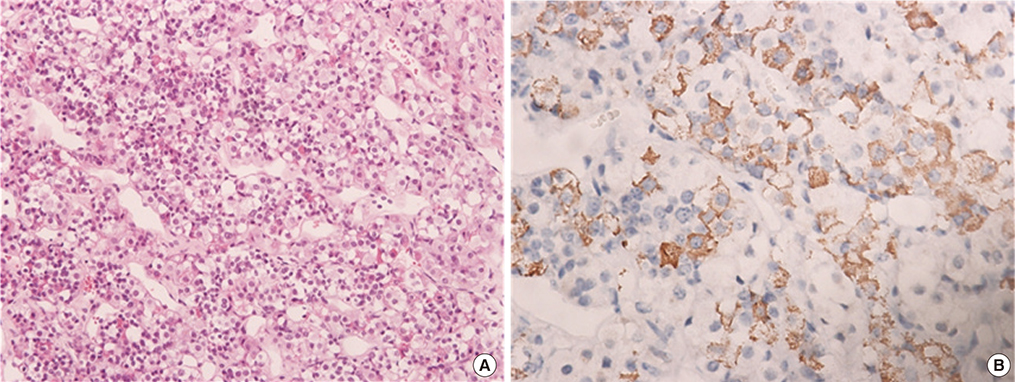
Fig. 5 Pathological findings of the pituitary tumor identified it as a growth hormone (GH)-secreting adenoma. (A) A pituitary adenoma in the pituitary gland (H&E stain, ×200). (B) Immunohistochemical staining of the pituitary tumor tissue showed that tumor cells were uniformly positive for GH (×400).
Reference
-
1. Mosca S, Paolillo S, Colao A, Bossone E, Cittadini A, Iudice FL, et al. Cardiovascular involvement in patients affected by acromegaly: an appraisal. Int J Cardiol. 2013; 167:1712–1718.2. Bihan H, Espinosa C, Valdes-Socin H, Salenave S, Young J, Levasseur S, et al. Long-term outcome of patients with acromegaly and congestive heart failure. J Clin Endocrinol Metab. 2004; 89:5308–5313.3. Lim DJ, Kwon HS, Cho JH, Kim SH, Choi YH, Yoon KH, et al. Acromegaly associated with type 2 diabetes showing normal IGF-1 levels under poorly controlled glycemia. Endocr J. 2007; 54:537–541.4. Arihara Z, Sakurai K, Yamada S, Murakami O, Takahashi K. Acromegaly with normal IGF-1 levels probably due to poorly controlled diabetes mellitus. Tohoku J Exp Med. 2008; 216:325–329.5. Ryu JS, Shong YK, Lee KU, Kim JJ, Park SW, Park SJ, et al. A case of acromegaly with dilated cardiomyopathy. J Korean Soc Endocrinol. 1990; 5:314–317.6. Minniti G, Moroni C, Jaffrain-Rea ML, Esposito V, Santoro A, Affricano C, et al. Marked improvement in cardiovascular function after successful transsphenoidal surgery in acromegalic patients. Clin Endocrinol (Oxf). 2001; 55:307–313.7. Grottoli S, Gasco V, Ragazzoni F, Ghigo E. Hormonal diagnosis of GH hypersecretory states. J Endocrinol Invest. 2003; 26:10 Suppl. 27–35.8. Dutta P, Das S, Bhansali A, Bhadada SK, Rajesh BV, Reddy KS, et al. Congestive heart failure in acromegaly: a review of 6 cases. Indian J Endocrinol Metab. 2012; 16:987–990.9. Ballintine EJ, Foxman S, Gorden P, Roth J. Rarity of diabetic retinopathy in patients with acromegaly. Arch Intern Med. 1981; 141:1625–1627.10. Payne JF, Tangpricha V, Cleveland J, Lynn MJ, Ray R, Srivastava SK. Serum insulin-like growth factor-I in diabetic retinopathy. Mol Vis. 2011; 17:2318–2324.11. Rymaszewski Z, Cohen RM, Chomczynski P. Human growth hormone stimulates proliferation of human retinal microvascular endothelial cells in vitro. Proc Natl Acad Sci U S A. 1991; 88:617–621.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Continuous Positive Airway Pressure Therapy in a Obstructive SleepApnea Syndrome associated with Active Acromegaly
- A Case of Acromegaly Associated with Lung and Gastric Cancer
- A Case of Acromegaly with Gall Bladder Cancer
- The Fascinating Interplay between Growth Hormone, Insulin-Like Growth Factor-1, and Insulin
- A Case of Acromegaly Presenting with Diabetic Ketoacidosis
