Ewha Med J.
2018 Jan;41(1):19-23. 10.12771/emj.2018.41.1.19.
Influence of the Phase of Menstrual Cycle on Postoperative Nausea and Vomiting after Breast Cancer Surgery
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Ewha Womans University College of Medicine, Seoul, Korea. kdyeon@ewha.ac.kr
- KMID: 2403019
- DOI: http://doi.org/10.12771/emj.2018.41.1.19
Abstract
OBJECTIVES
The phase of the menstrual cycle was demonstrated to have an influence on the incidence of postoperative nausea and vomiting (PONV) after gynecologic laparoscopic surgery, but little was known for breast surgery, which was shown to have relatively higher incidence of PONV, >60%. We performed this study to investigate the influence of the phase of menstrual cycle on PONV after breast cancer surgery.
METHODS
A total of 103 patients, who were scheduled for breast cancer surgery under general anesthesia, were recruited, and patients with irregular menstrual cycles, history of previous history of PONV were excluded. Groups were divided in two ways as follows: 1) gynecologic classification: premenstrual and menstrual (days 25 to 6), follicular (days 8 to 12), ovulation (days 13 to 15), and luteal phase (days 20 to 24); 2) menstrual classification: menstrual (days 1 to 8) and non-menstrual (days 9 to 28). PONV were recorded using Rhodes index of nausea, vomiting and retching at postoperative 6 and 24 hours.
RESULTS
The overall incidence of PONV during postoperative 24 hours was 35.4%. At the menstrual classification, the incidence of PONV at postoperative 24 hours was higher in the menstrual group than that in the non-menstrual group (16.7% vs. 4.2%, P=0.057). The severity of PONV, measured with Rhodes index of nausea, vomiting and retching was significantly different between menstrual and non-menstrual groups (P=0.034).
CONCLUSION
The duration and severity of the PONV after breast cancer surgery were demonstrated to be prolonged and aggravated during menstruation, respectively. Therefore, consideration of menstrual cycle for scheduling breast cancer surgery could effectively prevent the PONV and reduce medical cost.
MeSH Terms
Figure
-
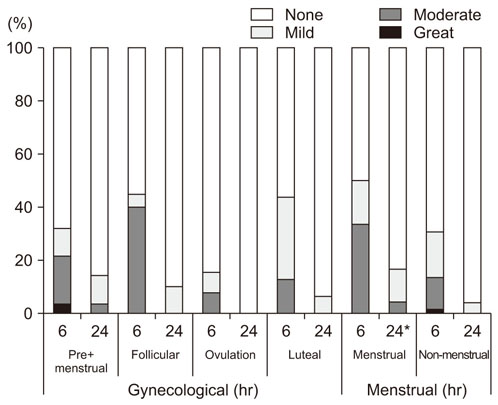
Fig. 1 The incidence and degree of postoperative nausea and vomiting at 6 and 24 hours after surgery. *P<0.05 compared to non-menstrual group.
Reference
-
1. Palazzo MG, Strunin L. Anaesthesia and emesis. I. Etiology. Can Anaesth Soc J. 1984; 31:178–187.
Article2. Andrews PL. Physiology of nausea and vomiting. Br J Anaesth. 1992; 69:7 Suppl 1. 2S–19S.
Article3. Harris JR, Lippman ME, Veronesi U, Willett W. Breast cancer (1). N Engl J Med. 1992; 327:319–328.4. Reihner E, Grunditz R, Giesecke K, Gustafsson LL. Postoperative nausea and vomiting after breast surgery: efficacy of prophylactic ondansetron and droperidol in a randomized placebo-controlled study. Eur J Anaesthesiol. 2000; 17:197–203.
Article5. Gan TJ, Diemunsch P, Habib AS, Kovac A, Kranke P, Meyer TA, et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2014; 118:85–113.
Article6. Honkavaara P, Lehtinen AM, Hovorka J, Korttila K. Nausea and vomiting after gynaecological laparoscopy depends upon the phase of the menstrual cycle. Can J Anaesth. 1991; 38:876–879.
Article7. Sener EB, Kocamanoglu S, Cetinkaya MB, Ustun E, Bildik E, Tur A. Effects of menstrual cycle on postoperative analgesic requirements, agitation, incidence of nausea and vomiting after gynecological laparoscopy. Gynecol Obstet Invest. 2005; 59:49–53.
Article8. Beattie WS, Lindblad T, Buckley DN, Forrest JB. The incidence of postoperative nausea and vomiting in women undergoing laparoscopy is influenced by the day of menstrual cycle. Can J Anaesth. 1991; 38:298–302.
Article9. Rhodes VA, McDaniel RW. The index of nausea, vomiting, and retching: a new format of the lndex of Nausea and Vomiting. Oncol Nurs Forum. 1999; 26:889–894.10. Suh JK, Bae DJ, Cho SY, Jeon WJ. The assessment of Postoperative Nausea and Vomiting (PONV) using rhodes index in PONV high risk group. Korean J Anesthesiol. 2008; 54:278–282.
Article11. Kapur PA. The big “little problem”. Anesth Analg. 1991; 73:243–245.12. Myles PS, Williams DL, Hendrata M, Anderson H, Weeks AM. Patient satisfaction after anaesthesia and surgery: results of a prospective survey of 10,811 patients. Br J Anaesth. 2000; 84:6–10.
Article13. Apfel CC, Laara E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999; 91:693–700.14. Divatia JV, Vaidya JS, Badwe RA, Hawaldar RW. Omission of nitrous oxide during anesthesia reduces the incidence of postoperative nausea and vomiting. A meta-analysis. Anesthesiology. 1996; 85:1055–1062.15. Overdyk FJ, Roy RC. If nitrous oxide induces emesis, maybe 100% oxygen is an antiemetic. Anesth Analg. 1997; 84:231–232.
Article16. Beattie WS, Lindblad T, Buckley DN, Forrest JB. Menstruation increases the risk of nausea and vomiting after laparoscopy: a prospective randomized study. Anesthesiology. 1993; 78:272–276.17. Tramer MR. A rational approach to the control of postoperative nausea and vomiting: evidence from systematic reviews. Part I. Efficacy and harm of antiemetic interventions, and methodological issues. Acta Anaesthesiol Scand. 2001; 45:4–13.
