J Korean Acad Oral Health.
2017 Dec;41(4):231-236. 10.11149/jkaoh.2017.41.4.231.
Changes in bisphenol A concentrations in urine according to sealant filling in children
- Affiliations
-
- 1Department of Preventive Dentistry, School of Dentistry, Kyungpook National University, Daegu, Korea. cyh1001@knu.ac.kr
- 2Department of Dental Hygiene, Choonhae College of Health Sciences, Ulsan, Korea.
- KMID: 2400237
- DOI: http://doi.org/10.11149/jkaoh.2017.41.4.231
Abstract
OBJECTIVES
The objectives of this study were to investigate the changes in bisphenol A (BPA) concentrations in urine from before to after sealant filling and the relationship between BPA and the number of teeth with sealed surfaces.
METHODS
Thirty-one children aged 6 and 7 years from three elementary schools in Daegu city who did not have any sealant and resin filling were selected as subjects. Urine samples were collected before and after sealant filling until 24 hours, with informed consent from their caregivers. The BPA concentration in all the collected urine samples was analyzed at Seegene Medical. Statistical analysis was performed using the Friedman test, Scheirer-Ray-Hope test, and the repeated-measures generalized linear mixed model of SPSS version 22.0.
RESULTS
The BPA concentrations increased from 3.49-μg/g creatinine before to 4.91-μg/g creatinine 2-3 hours later and to 4.15-μg/g creatinine after 24 hours. The more teeth with sealed surfaces, the higher the BPA concentration in children, but the difference was not statistically significant (P>0.05).
CONCLUSIONS
The BPA concentrations were highest at 2-3 hours after sealant filling and decreased at 24 hours. Exposure to the sealant appears to have a meaningful correlation with the concentration of BPA in the urine of children.
Keyword
Figure
-
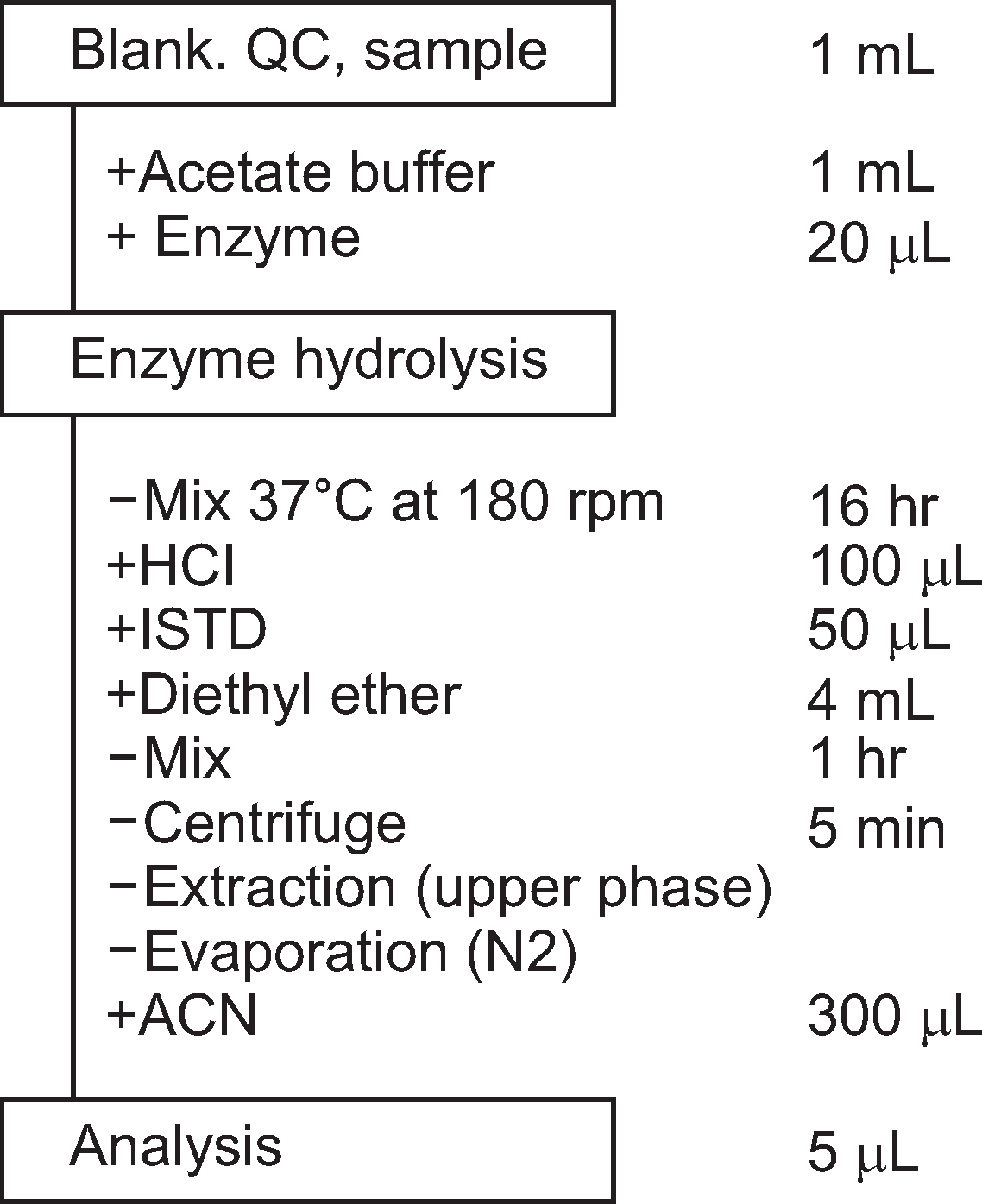
Fig. 1. Urine sample preparation.
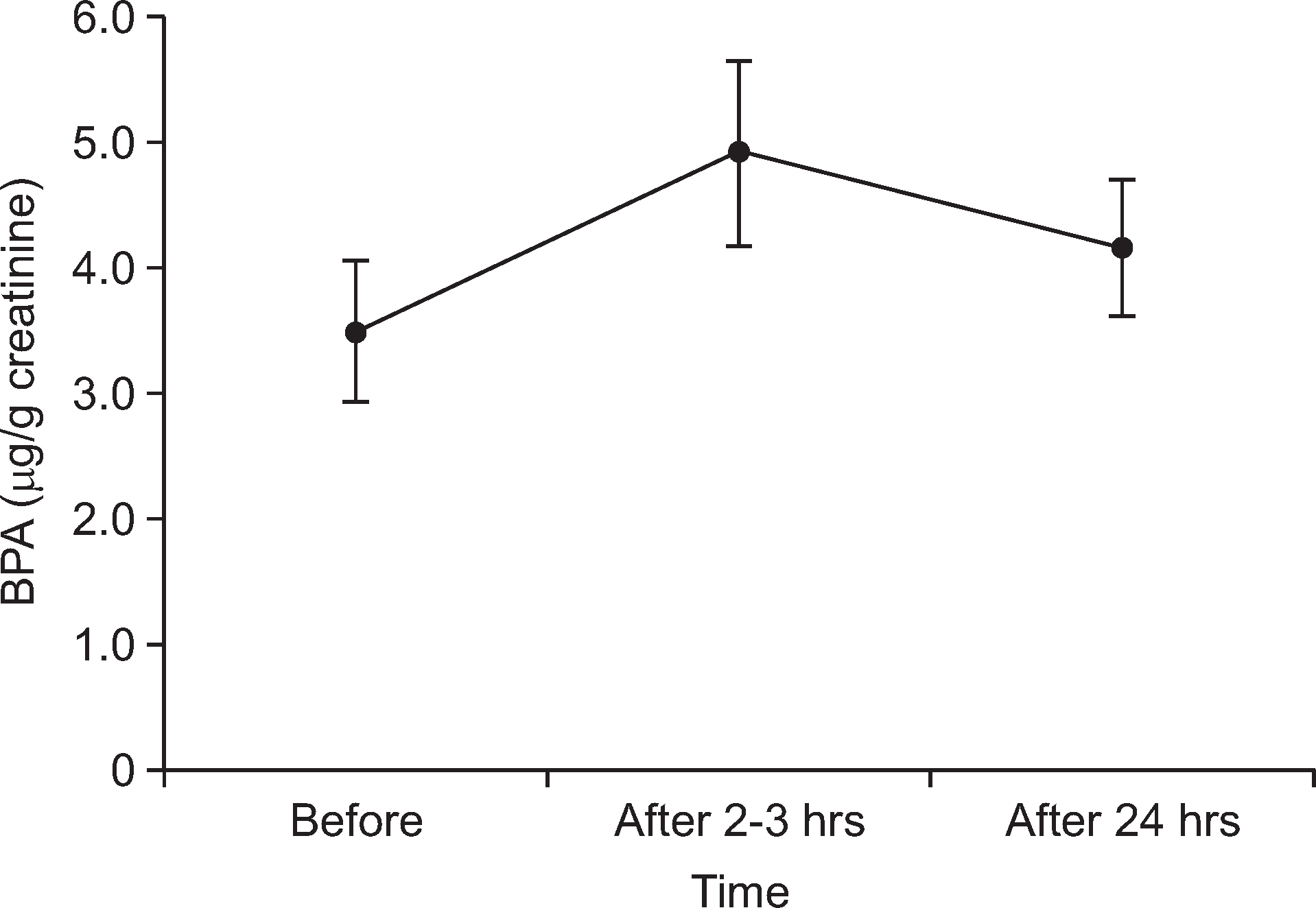
Fig. 2. Change of creatinine adjusted BPA concentrations before and after sealant restoration.

Fig. 3. Change of creatinine adjusted BPA concentrations according to the number of sealant surfaces.
Reference
-
References
1. Kang BW, Kim KS. 5th Preventive dentistry. 5th ed.Seoul: Koonja;2015. p. 25–48.2. Menaker L, Morhart RE, Navia JM. The biologic basis of dental caries. London: Harper and Row publishers Inc;1979. p. 461–481.3. Newbrun E. Cariology 3rd. Chicago: Quintessence;1989. p. 315.4. Horowitz AM. Effective oral health education and promotion programs to prevent dental caries. Int Dent J. 1983; 33:171–181.5. Beauchamp J, Caufield PW, Donly KJ, Feigal R, Gooch B, Ismail A, et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc,. 2008; 139:257–268.
Article6. Park KH, Shin SC. A Clinical study on the retention rate of pit & fissure sealing. J Korean Acad Oral Health. 1993; 17:53–68.7. Korea Institute for Health and Social Affairs. 2007 report of oral health services. Seoul: Korea Institute for Health and Social Af-fairs;2008. p. 92–94.8. Korea Ministry of Government Legislation. Legislation search, concerning standard of medical care expenses on national health insurance [Internet]. [cited 2016 Nov 07]. Available from. http://www.law.go.kr/lsSc.do?menuId=0&p1=&subMenu=1&nwYn=1§ion=&query=%EA%B5%AC%EA%B0%95%EB%B3%B4%EA%B1%B4%EB%B2%95&x=0&y=0#liBgcolor5.9. Ministry of Health and Welfare. 2015 Korean children’s oral health survey. Sejong: Ministry of Health & Welfare;2016. p. 147–148.10. Fung EY, Ewoldson NO, Germain HAS, Marx DB, Miaw CL, Siew C, et al. Pharmacokinetics of bisphenol A released from a dental sealant. J Am Dent Assoc. 2000; 131:51–58.
Article11. von Goetz N, Wormuth M, Scheringer M, Hungerbuhler K. Bisphe-nol A: how the most relevant exposure sources contribute to total consumer exposure. Risk Anal. 2010; 30:473–487.
Article12. Trasande L, Attina TM, Blustein J. Association between urinary bisphenol A concentration and obesity prevalence in children and adolescents. J Am Med Assoc. 2012; 308:1113–1121.
Article13. Trasande L, Attina TM, Trachtman H. Bisphenol A exposure is associated with low-grade urinary albumin excretion in children of the United States. Kidney Int. 2013; 83:741–748.
Article14. Maserejian NN, Trachtenberg FL, Hauser R, McKinlay S, Shrader P, Tavares M, et al. Dental composite restorations and psychosocial function in children. Am Acad Pediatr. 2012; 130:e328–e338.
Article15. Stahlhut RW, Welshons WV, Swan SH. Bisphenol A data in NHANES suggest longer than expected half-life, substantial non food exposure, or both. Environ Health Perspect. 2009; 117:784–789.16. Maserejian NN, Hauser R, Tavares M, Trachtenberg FL, Shrader P, McKinlay S. Dental composites and amalgam and physical development in children. J Dent Res. 2012; 91:1019–1025.
Article17. Kim EK, Choi YH. Impact of the sealant on salivary and urinary bisphenol-A concentration in children. J Dent Hyg Sci. 2015; 15:32–37.
Article18. Chung SY, Kwon H, Choi YH, Karmaus W, Merchant AT, Song KB, et al. Dental composite fillings and bisphenol A among children: a survey in South Korea. Int Dent J. 2012; 62:65–69.
Article19. Joskow R, Barr DB, Barr JR, Calafat AM, Needham LL, Rubin C. Exposure to bisphenol A from bis-glycidyl dimethacrylate-based dental sealants. J Am Dent Assoc. 2006; 137:353–362.
Article20. Hill RH, Ashley DL, Head SL, Needham LL, Pirkle JL. p-Dichlorobenzene exposure among 1,000 adults in the United States. Arch Environ Health. 1995; 50:277–280.21. Health Canada. Health risk assessment of bisphenol A from food packaging applications. Ottawa: Health Canada;2008.22. Taylor JA, Welshons WV, Vom Saal FS. No effect of route of exposure (oral;subcutaneous injection) on plasma bisphenol A throughout 24 h after administration in neonatal female mice. Reprod Toxi-col. 2008; 25:169–176.23. Martin MD, Bajet D, Woods JS, Dills RL, Poulten EJ. Detection of dental composite and sealant resin components in urine. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2005; 99:429.
Article24. Kingman A, Hyman J, Masten SA, Jayaram B, Smith C, Eichmiller F, et al. Bisphenol A and other compounds in human saliva and urine associated with the placement of composite restorations. J Am Dent Assoc. 2012; 143:1292–1302.
Article25. Zimmerman-Downs JM, Shuman D, Stull SC, Ratzlaff RE. Bisphenol A blood and saliva levels prior to and after dental sealant placement in adults. J Dent Hyg. 2010; 84:145–150.26. Yi SK. Salivary bisphenol-A level related with composite resin restoration [Master’s thesis]. Pusan: Pusan National University;2016. [Korean].27. van Landuyt KL, Nawrot T, Geebelen B, De Munck J, Snauwaert J, Yoshihara K, et al. How much do resin-based dental materials release? A meta-analytical approach. Dental Materials. 2011; 27:723–747.
Article28. Rueggeberg FA, Dlugokinski M, Ergle JW. Minimizing patients exposure to uncured components in a dental sealant. J Am Dent Assoc. 1999; 130:1751–1757.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Salivary Bisphenol-A Levels due to Dental Sealant/Resin: A Case-Control Study in Korean Children
- Associations Between Thyroid Hormone Levels and Urinary Concentrations of Bisphenol A, F, and S in 6-Year-old Children in Korea
- Experimental Study on the Effect of Fibrin Sealant in Renal Surgery
- Analysis of the Characteristics of Children and Adolescent Patients Received Sealant after National Health Insurance Coverage using Big Data
- Antibacterial Efficacy of Dental Sealant Containing Phytoncide
