Metaplastic Carcinoma with Chondroid Differentiation Arising in Microglandular Adenosis
- Affiliations
-
- 1Department of Pathology, Chonnam National University Medical School, Gwangju, Korea. jshinlee@hanmail.net
- 2Department of Surgery, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2392583
- DOI: http://doi.org/10.4132/jptm.2016.10.06
Abstract
- Microglandular adenosis (MGA) of the breast is a rare, benign proliferative lesion but with a significant rate of associated carcinoma. Herein, we report an unusual case of metaplastic carcinoma with chondroid differentiation associated with typical MGA. Histologically, MGA showed a direct transition to metaplastic carcinoma without an intervening atypical MGA or ductal carcinoma in situ component. The immunohistochemical profile of the metaplastic carcinoma was mostly similar to that of MGA. In both areas, all the epithelial cells were positive for S-100 protein, but negative for estrogen receptor, progesterone receptor, HER2/neu, and epidermal growth factor receptor. An increase in the Ki-67 and p53 labelling index was observed from MGA to invasive carcinoma. To the best of our knowledge, this is the first case of metaplastic carcinoma with chondroid differentiation arising in MGA in Korea. This case supports the hypothesis that a subset of MGA may be a non-obligate morphologic precursor of breast carcinoma, especially the triple-negative subtype.
MeSH Terms
Figure
-
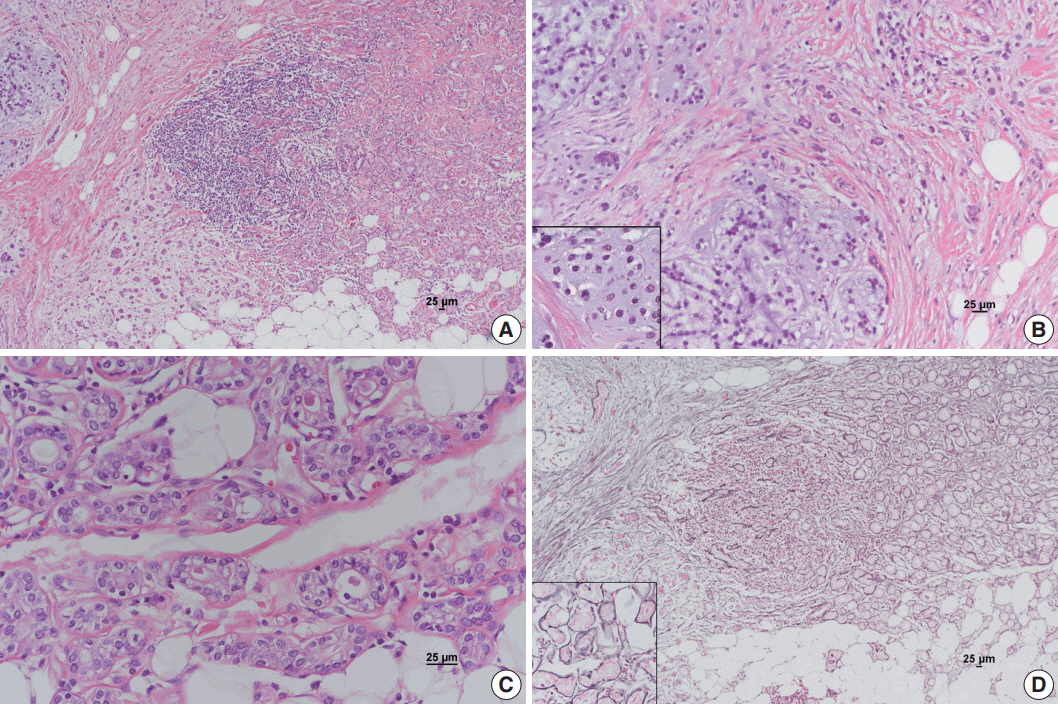
Fig. 1. Metaplastic carcinoma with mesenchymal differentiation arising in microglandular adenosis (MGA). (A) MGA on the right shows direct transition to invasive carcinoma on the left. (B) Invasive carcinoma primarily composed of cord-like cells scattered in the chondromyxoid matrix with focal chondroid differentiation (inset). (C) Typical glands in MGA are lined by uniform cuboidal cells regularly spaced around a lumen containing a colloid-like secretion. (D) Basement membranes highlighted by the reticulin stain are preserved in the MGA area (inset) but disrupted in the invasive carcinoma area.
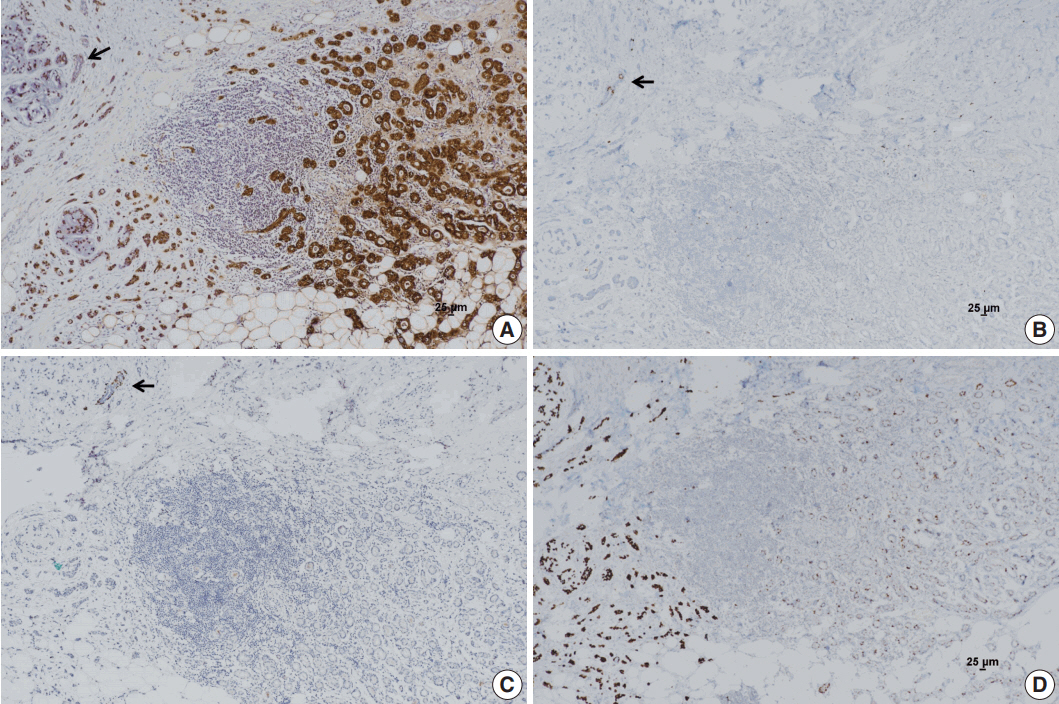
Fig. 2. Immunohistochemical stains. (A) S-100 protein is strongly positive in microglandular adenosis (MGA) and invasive carcinoma. Entrapped normal mammary gland is negative for S-100 protein (arrow). (B) Estrogen receptor (ER) is positive in entrapped normal mammary glands (arrow); however, MGA and invasive carcinoma are negative for ER. (C) No immunoreactivity for p63 is observed in the MGA area or invasive carcinoma area. Normal mammary glands are stained positively in myoepithelial cells (arrow). (D) An increase in p53 labelling index is observed from MGA to invasive carcinoma.
Reference
-
1. Shin SJ, Gobbi H. Microglandular adenosis, atypical microglandular adenosis and microglandular adenosis with carcinoma. In : Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, editors. WHO classification of tumours of the breast. 4th ed. Lyon: IARC Press;2012. p. 113–4.2. Brogi E. Adenosis and microglandular adenosis. In : Hoda SA, Brogi E, Koerner FC, Rosen PP, editors. Rosen’s breast pathology. 4th ed. Philadelphia: Lippincott Williams & Wilkins;2014. p. 183–212.3. James BA, Cranor ML, Rosen PP. Carcinoma of the breast arising in microglandular adenosis. Am J Clin Pathol. 1993; 100:507–13.
Article4. Koenig C, Dadmanesh F, Bratthauer GL, Tavassoli FA. Carcinoma arising in microglandular adenosis: an immunohistochemical analysis of 20 intraepithelial and invasive neoplasms. Int J Surg Pathol. 2000; 8:303–15.
Article5. Khalifeh IM, Albarracin C, Diaz LK, et al. Clinical, histopathologic, and immunohistochemical features of microglandular adenosis and transition into in situ and invasive carcinoma. Am J Surg Pathol. 2008; 32:544–52.
Article6. Shui R, Bi R, Cheng Y, Lu H, Wang J, Yang W. Matrix-producing carcinoma of the breast in the Chinese population: a clinicopathological study of 13 cases. Pathol Int. 2011; 61:415–22.
Article7. Zhong F, Bi R, Yu B, et al. Carcinoma arising in microglandular adenosis of the breast: triple negative phenotype with variable morphology. Int J Clin Exp Pathol. 2014; 7:6149–56.8. Liu LY, Sheng SH, Zhang ZY, Xu JH. A case of matrix-producing carcinoma of the breast with micoglandular adenosis and review of literature. Int J Clin Exp Pathol. 2015; 8:8568–72.9. Choi JE, Bae YK. Invasive breast carcinoma arising in microglandular adenosis: two case reports. J Breast Cancer. 2013; 16:432–7.
Article10. Shin SJ, Simpson PT, Da Silva L, et al. Molecular evidence for progression of microglandular adenosis (MGA) to invasive carcinoma. Am J Surg Pathol. 2009; 33:496–504.
Article11. Guerini-Rocco E, Piscuoglio S, Ng CK, et al. Microglandular adenosis associated with triple-negative breast cancer is a neoplastic lesion of triple-negative phenotype harbouring TP53 somatic mutations. J Pathol. 2016; 238:677–88.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mammary Carcinoma Arising in Microglandular Adenosis: A Report of Five Cases
- Ductal Carcinoma In Situ of the Breast Arising in Microglandular Adenosis
- Metaplastic Carcinoma with Chondroid Differentiation Mimicking Malignant Phyllodes Tumor: A Case Report
- Imaging Findings of Metaplastic Breast Carcinoma with Chondroid Differentiation: A Case Reports
- Metaplastic Carcinoma of the Breast with Chondroid Calcification: A Case Report
