Korean J Gastroenterol.
2017 Sep;70(3):145-149. 10.4166/kjg.2017.70.3.145.
Pneumoretroperitoneum, Pneumomediastinum, Pneumothorax, and Subcutaneous Emphysema after Diagnostic Colonoscopy
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University School of Medicine, Daejeon, Korea. mhs1357@cnuh.co.kr
- KMID: 2390793
- DOI: http://doi.org/10.4166/kjg.2017.70.3.145
Abstract
- Colonoscopy is a commonly performed endoscopic procedure. Although it is generally considered to be safe, serious complications, such as colorectal perforation, can occur. Most colonic perforations are intraperitoneal and cause pneumoperitoneum with acute abdominal pain as the initial symptom. However, extraperitoneal perforations with pneumoretroperitoneum may happen, albeit rarely, with atypical initial symptoms. We report a rare case of rectosigmoid perforation occurring after diagnostic colonoscopy that developed into pneumoretroperitoneum, pneumomediastinum, pneumothorax, and subcutaneous emphysema, with a change in voice and neck swelling as the initial symptoms. The patient was successfully treated with endoscopic closure of the perforation and conservative management.
MeSH Terms
Figure
-
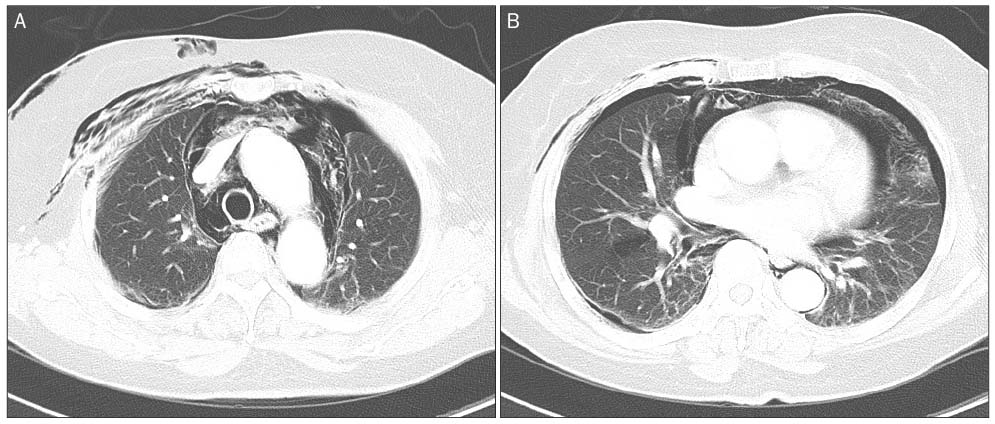
Fig. 1 Contrast-enhanced computed tomography of the chest showing. (A) Pneumomediastinum, subcutaneous emphysema. (B) Pneumothorax.

Fig. 2 Erect abdominal x-ray showing pneumoretroperitoneum.

Fig. 3 Lateral neck x-ray showing prevertebral air and subcutaneous emphysema around the neck.
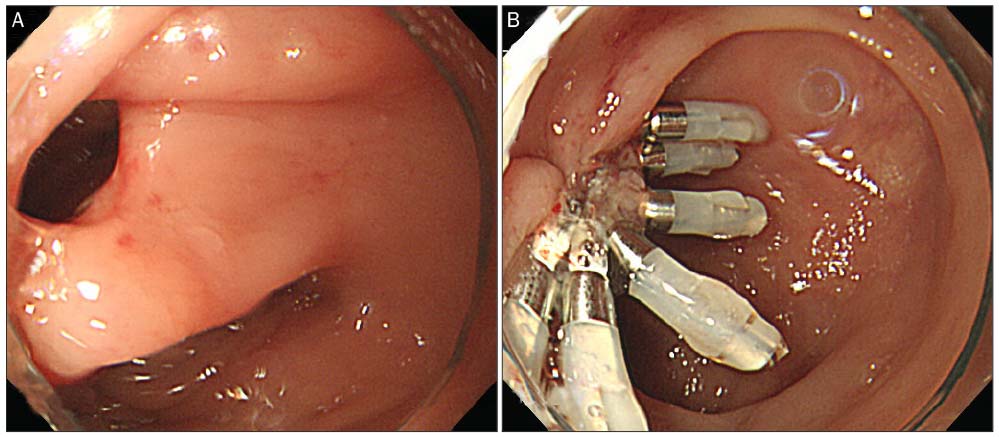
Fig. 4 Colonocopic finding. (A) The perforation was found at the rectosigmoid colon. (B) Endoscopic clipping was performed to close the perforation.
Reference
-
1. ASGE Standards of Practice Committee. Fisher DA, Maple JT, et al. Complications of colonoscopy. Gastrointest Endosc. 2011; 74:745–752.2. Panteris V, Haringsma J, Kuipers EJ. Colonoscopy perforation rate, mechanisms and outcome: from diagnostic to therapeutic colonoscopy. Endoscopy. 2009; 41:941–951.3. Singh JP, Steward MJ, Booth TC, Mukhtar H, Murray D. Evolution of imaging for abdominal perforation. Ann R Coll Surg Engl. 2010; 92:182–188.4. Jung HC, Kim HJ, Ji SB, et al. Pneumoretroperitoneum, pneumomediastinum, subcutaneous emphysema after a rectal endoscopic mucosal resection. Ann Coloproctol. 2016; 32:234–238.5. Lohsiriwat V. Colonoscopic perforation: incidence, risk factors, management and outcome. World J Gastroenterol. 2010; 16:425–430.6. Iqbal CW, Cullinane DC, Schiller HJ, Sawyer MD, Zietlow SP, Farley DR. Surgical management and outcomes of 165 colonoscopic perforations from a single institution. Arch Surg. 2008; 143:701–706. discussion 706-707.7. Lüning TH, Keemers-Gels ME, Barendregt WB, Tan AC, Rosman C. Colonoscopic perforations: a review of 30,366 patients. Surg Endosc. 2007; 21:994–997.8. Ko CW, Dominitz JA. Complications of colonoscopy: magnitude and management. Gastrointest Endosc Clin N Am. 2010; 20:659–671.9. Kim HH, Park SJ, Lee SH, et al. Efficacy of endoscopic submucosal resection with a ligation device for removing small rectal carcinoid tumor compared with endoscopic mucosal resection: analysis of 100 cases. Dig Endosc. 2012; 24:159–163.10. Ignjatović M, Jović J. Tension pneumothorax, pneumoretroperitoneum, and subcutaneous emphysema after colonoscopic polypectomy: a case report and review of the literature. Langenbecks Arch Surg. 2009; 394:185–189.11. Zeno BR, Shan SA. Colonoscopy-associated pneumothorax: a case of tension pneumothorax and review of the literature. Am J Med Sci. 2006; 332:153–155.12. Levy I, Gralnek IM. Complications of diagnostic colonoscopy, upper endoscopy, and enteroscopy. Best Pract Res Clin Gastroenterol. 2016; 30:705–718.13. Ho HC, Burchell S, Morris P, Yu M. Colon perforation, bilateral pneumothoraces, pneumopericardium, pneumomediastinum, and subcutaneous emphysema complicating endoscopic polypectomy: anatomic and management considerations. Am Surg. 1996; 62:770–774.14. Webb T. Pneumothorax and pneumomediastinum during colonoscopy. Anaesth Intensive Care. 1998; 26:302–304.15. Ball CG, Kirkpatrick AW, Mackenzie S, et al. Tension pneumothorax secondary to colonic perforation during diagnostic colonoscopy: report of a case. Surg Today. 2006; 36:478–480.16. Maunder RJ, Pierson DJ, Hudson LD. Subcutaneous and mediastinal emphysema. Pathophysiology diagnosis, and management. Arch Intern Med. 1984; 144:1447–1453.17. Tiwari A, Sharma H, Qamar K, Sodeman T, Nawras A. Recognition of extraperitoneal colonic perforation following colonoscopy: a review of the literature. Case Rep Gastroenterol. 2017; 11:256–264.18. Marwan K, Farmer KC, Varley C, Chapple KS. Pneumothorax, pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum and subcutaneous emphysema following diagnostic colonoscopy. Ann R Coll Surg Engl. 2007; 89:W20–W21.19. Kim BH, Yoon SJ, Lee JY, Moon JE, Chung IS. Subcutaneous emphysema, pneumomediastinum, pneumoretroperitoneum, and pneumoperitoneum secondary to colonic perforation during colonoscopy. Korean J Anesthesiol. 2013; 65:6 Suppl. S103–S104.20. Anyfantakis D, Kastanakis M, Karona P, Papadomichelakis A, Bobolakis E. Subcutaneous facial and neck emphysema as first sign of intestinal perforation in a female patient after a routine colonoscopy. Eurasian J Med. 2016; 48:230–232.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pneumothorax, Pneumomediastinum, Subcutaneous Emphysema, Pneumoretroperitoneum Secondary to Colonoscopic Perforation
- Pneumoretroperitoneum, Pneumomediastinum, Peumopericardium, and Subcutaneous Emphysema after Colonoscopic Examination
- Pneumoretroperitoneum, Pneumomediastinum, Subcutaneous Emphysema After a Rectal Endoscopic Mucosal Resection
- Pneumomediastinum and Subcutaneous Emphysema after Use of a High-Speed Dental Handpiece
- Subcutaneous emphysema, pneumomediastinum, pneumoretroperitoneum, and pneumoperitoneum secondary to colonic perforation during colonoscopy
