Ann Dermatol.
2016 Oct;28(5):569-574. 10.5021/ad.2016.28.5.569.
A Comparative Study of Oral Cyclosporine and Betamethasone Minipulse Therapy in the Treatment of Alopecia Areata
- Affiliations
-
- 1Department of Dermatology, Kyungpook National University School of Medicine, Daegu, Korea. kimdw@knu.ac.kr
- KMID: 2382880
- DOI: http://doi.org/10.5021/ad.2016.28.5.569
Abstract
- BACKGROUND
Various systemic agents have been assessed for the treatment of alopecia areata (AA); however, there is a paucity of comparative studies.
OBJECTIVE
To assess and compare cyclosporine and betamethasone minipulse therapy as treatments for AA with regard to effectiveness and safety.
METHODS
Data were collected from 88 patients who received at least 3 months of oral cyclosporine (n=51) or betamethasone minipulse therapy (n=37) for AA. Patients with ≥50% of terminal hair regrowth in the alopecic area were considered responders.
RESULTS
The responder of the cyclosporine group was 54.9% and that of the betamethasone minipulse group was 37.8%. In the cyclosporine group, patients with mild AA were found to respond better to the treatment. Based on the patient self-assessments, 70.6% of patients in the cyclosporine group and 43.2% of patients in the betamethasone minipulse group rated their hair regrowth as excellent or good. Side effects were less frequent in the cyclosporine group.
CONCLUSION
Oral cyclosporine appeared to be superior to betamethasone minipulse therapy in terms of treatment effectiveness and safety.
MeSH Terms
Figure
-
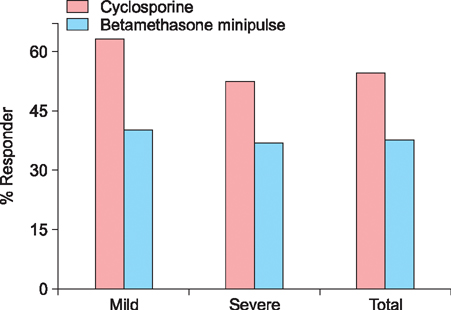
Fig. 1 Treatment responses according to the extent of alopecia at baseline. AA: alopecia areata, AT: alopecia totalis, AU: alopecia universalis. Extent of alopecia at baseline: mild AA: S1 (<25% scalp hair loss), S2 (25%~49%). Severe AA: S3 (50%~74%), S4 (75%~99%), AT, AU.
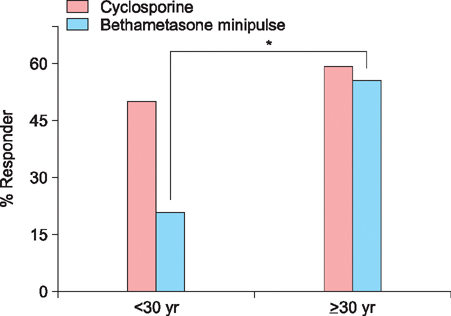
Fig. 2 Treatment responses according to age at onset. Onset age of AA: early-onset AA: <30 years at the onset of AA, late-onset AA: ≥30 years at the onset of AA. *p<0.05.
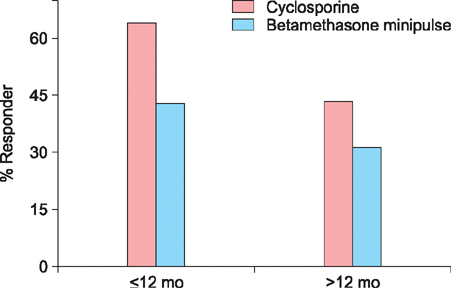
Fig. 3 Treatment responses according to duration of disease.
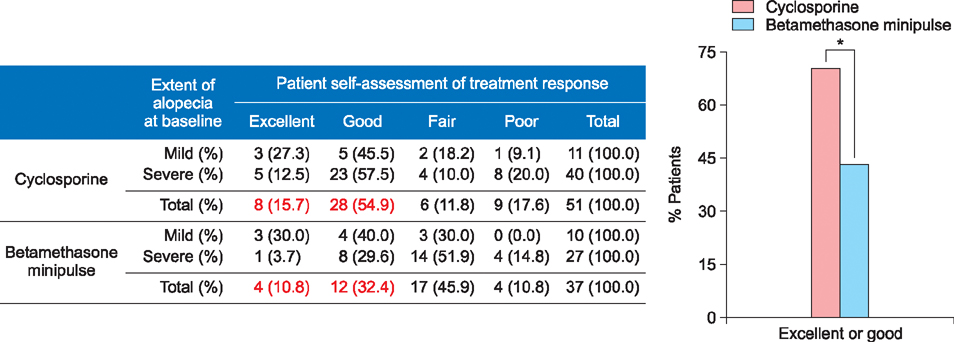
Fig. 4 Patient self-assessments of treatment responses. *p<0.05.
Reference
-
1. Amor KT, Ryan C, Menter A. The use of cyclosporine in dermatology: part I. J Am Acad Dermatol. 2010; 63:925–946. quiz 947-948.
Article2. Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J. Alopecia areata update: part II. Treatment. J Am Acad Dermatol. 2010; 62:191–202. quiz 203-204.3. Yang CC, Lee CT, Hsu CK, Lee YP, Wong TW, Chao SC, et al. Early intervention with high-dose steroid pulse therapy prolongs disease-free interval of severe alopecia areata: a retrospective study. Ann Dermatol. 2013; 25:471–474.
Article4. Kar BR, Handa S, Dogra S, Kumar B. Placebo-controlled oral pulse prednisolone therapy in alopecia areata. J Am Acad Dermatol. 2005; 52:287–290.
Article5. Kurosawa M, Nakagawa S, Mizuashi M, Sasaki Y, Kawamura M, Saito M, et al. A comparison of the efficacy, relapse rate and side effects among three modalities of systemic corticosteroid therapy for alopecia areata. Dermatology. 2006; 212:361–365.
Article6. Lester RS, Knowles SR, Shear NH. The risks of systemic corticosteroid use. Dermatol Clin. 1998; 16:277–288.
Article7. Khaitan BK, Mittal R, Verma KK. Extensive alopecia areata treated with betamethasone oral mini-pulse therapy: an open uncontrolled study. Indian J Dermatol Venereol Leprol. 2004; 70:350–353.8. Sharma VK, Gupta S. Twice weekly 5 mg dexamethasone oral pulse in the treatment of extensive alopecia areata. J Dermatol. 1999; 26:562–565.
Article9. Deshpande D, Dhurat R, Saraogi P, Mishra S, Nayak C. Extensive alopecia areata: not necessarily recalcitrant to therapy. Int J Trichology. 2011; 3:80–83.
Article10. Friedli A, Labarthe MP, Engelhardt E, Feldmann R, Salomon D, Saurat JH. Pulse methylprednisolone therapy for severe alopecia areata: an open prospective study of 45 patients. J Am Acad Dermatol. 1998; 39:597–602.
Article11. Kahan BD. Cyclosporine. N Engl J Med. 1989; 321:1725–1738.
Article12. Taylor M, Ashcroft AT, Messenger AG. Cyclosporin A prolongs human hair growth in vitro. J Invest Dermatol. 1993; 100:237–239.
Article13. Gupta AK, Ellis CN, Nickoloff BJ, Goldfarb MT, Ho VC, Rocher LL, et al. Oral cyclosporine in the treatment of inflammatory and noninflammatory dermatoses. A clinical and immunopathologic analysis. Arch Dermatol. 1990; 126:339–350.
Article14. Gupta AK, Ellis CN, Cooper KD, Nickoloff BJ, Ho VC, Chan LS, et al. Oral cyclosporine for the treatment of alopecia areata. A clinical and immunohistochemical analysis. J Am Acad Dermatol. 1990; 22:242–250.15. Park J, Yoo KH, Rho YK, Han TY, Li K, Seo SJ, et al. Comparison of therapeutic effect of high dose corticosteroid pulse therapy and combination therapy of cyclosporine with low does corticosteroid for severe alopecia areata. Korean J Dermatol. 2009; 47:1220–1226.16. Sharma VK. Pulsed administration of corticosteroids in the treatment of alopecia areata. Int J Dermatol. 1996; 35:133–136.
Article17. Jang JW, Kim DW, Jun JB, Chung SL. Oral minipulse therapy with betamethasone in the treatment of alopecia areata. Korean J Dermatol. 2001; 39:775–781.18. Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J. Alopecia areata update: part I. Clinical picture, histopathology, and pathogenesis. J Am Acad Dermatol. 2010; 62:177–188. quiz 189-190.19. Wasserman D, Guzman-Sanchez DA, Scott K, McMichael A. Alopecia areata. Int J Dermatol. 2007; 46:121–131.
Article20. Kim BJ, Min SU, Park KY, Choi JW, Park SW, Youn SW, et al. Combination therapy of cyclosporine and methylprednisolone on severe alopecia areata. J Dermatolog Treat. 2008; 19:216–220.
Article21. Tosti A, Bellavista S, Iorizzo M. Alopecia areata: a long term follow-up study of 191 patients. J Am Acad Dermatol. 2006; 55:438–441.
Article22. Madani S, Shapiro J. Alopecia areata update. J Am Acad Dermatol. 2000; 42:549–566. quiz 567-570.
Article23. Lew BL, Shin MK, Sim WY. Acute diffuse and total alopecia: A new subtype of alopecia areata with a favorable prognosis. J Am Acad Dermatol. 2009; 60:85–93.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Oral Minipulse Therapy with Betamethasone in the Treatment of Alopecia Areata
- A Case of Alopecia Areata in a Patient taking Cyclosporine
- Cyclosporine Combination Therapy in Alopecia Areata
- A Case of Congenitally Developed Alopecia Areata
- Comparison of Therapeutic Effect of High Dose Corticosteroid Pulse Therapy and Combination Therapy of Cyclosporine with Low Does Corticosteroid for Severe Alopecia Areata
