A Metastatic Lung Adnocarcinoma Misdiagnosed as Trauma Induced Sternoclavicular Joint Arthrosis
- Affiliations
-
- 1Orthopaedic Oncology Clinic, National Cancer Center, Goyang, Korea.
- 2Department of Orthopedic Surgery, Myongji Hospital, Seonam University College of Medicine, Goyang, Korea. doctoryub@naver.com
- KMID: 2382057
- DOI: http://doi.org/10.5763/kjsm.2016.34.2.181
Abstract
- The prevalence of metastatic tumorous lesion at medial clavicle or sternoclavicular joint is low. Herein, we presented a 45-year-old female patient with left sternoclavicular joint pain followed a weight-lifting exercise. The patient was initially diagnosed as traumatic sternoclavicular arthrosis, however, on later computed tomography scan demonstrated the bony destruction of medial clavicle which was diagnosed as metastasized non-small cell lung carcinoma after a fine needle biopsy.
Keyword
MeSH Terms
Figure
-

Fig. 1. No specific abnormality was observed on clavicular X-ray at first visit (A). However, the periarticular soft tissue swelling with subcutaneous fat infiltration was observed at left sternoclavicular joint (white arrow) (B).
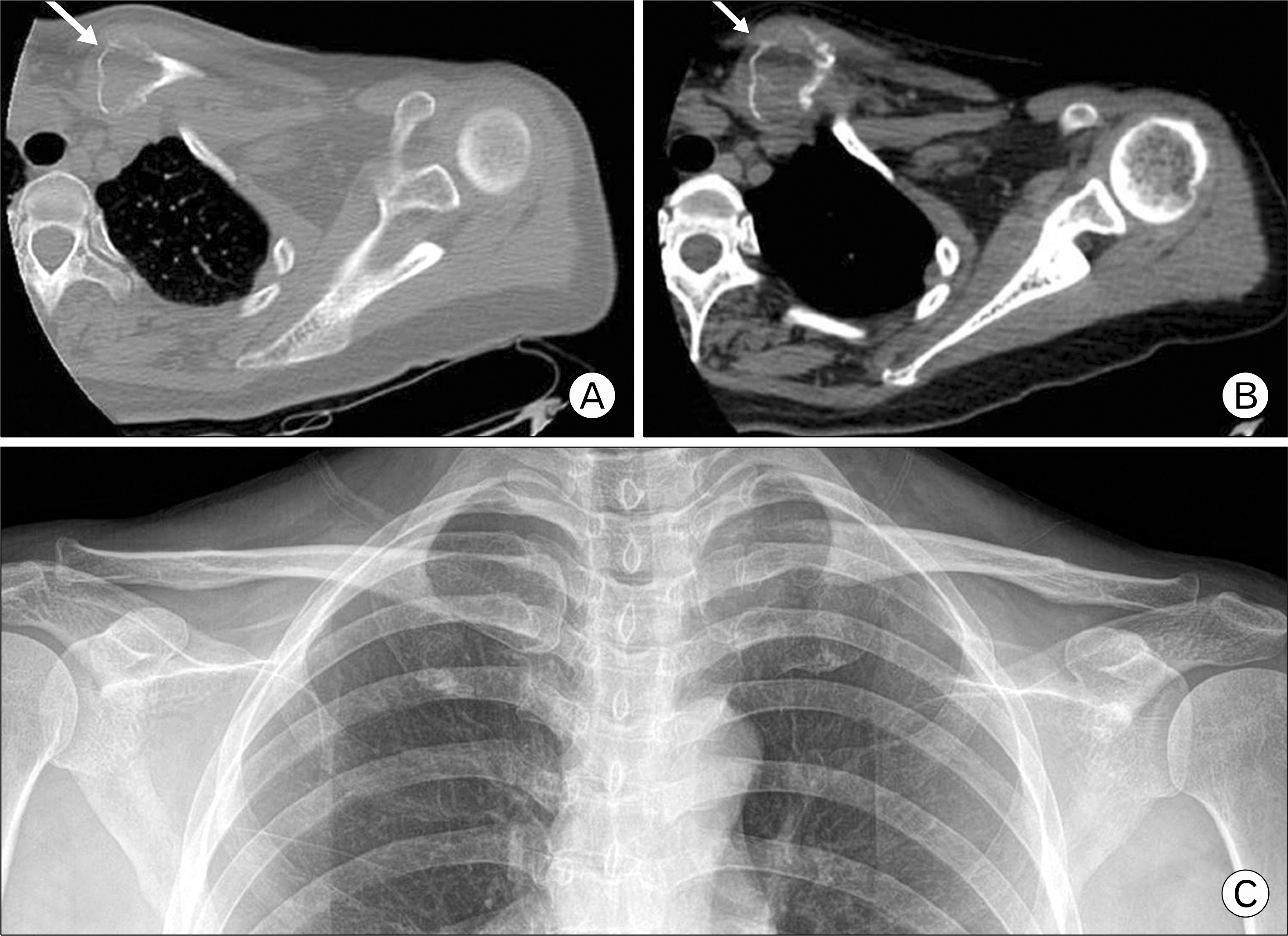
Fig. 2. The periarticular soft tissue swelling with subcutaneous fat infiltration was observed at left sternoclavicular joint after 2 month (white arrow) (A). With 2-month interval, the osterolysis with sternoclavicular joint destruction was progressed rapidly (white arrow) (B). The destructive pattern of medial clavicle was observed at 4-month follow-up after the first visit (C).
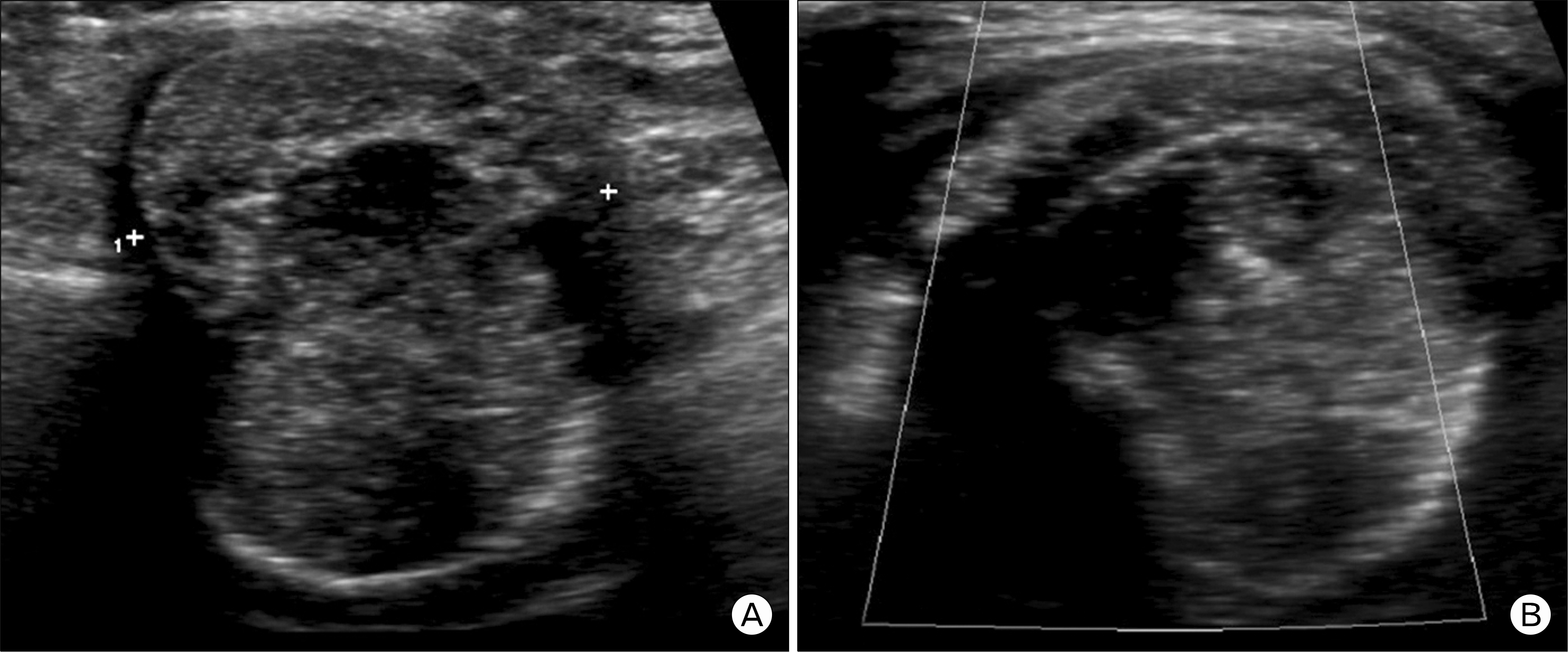
Fig. 3. A bony expansile and osteolytic solid mass lesion with heterogenity on medial end of left clavicle with 3.1×3.6×2.8 cm size was observed on ultrasonography (A) and no intralesional vascularity was observed by color Doppler study (B).
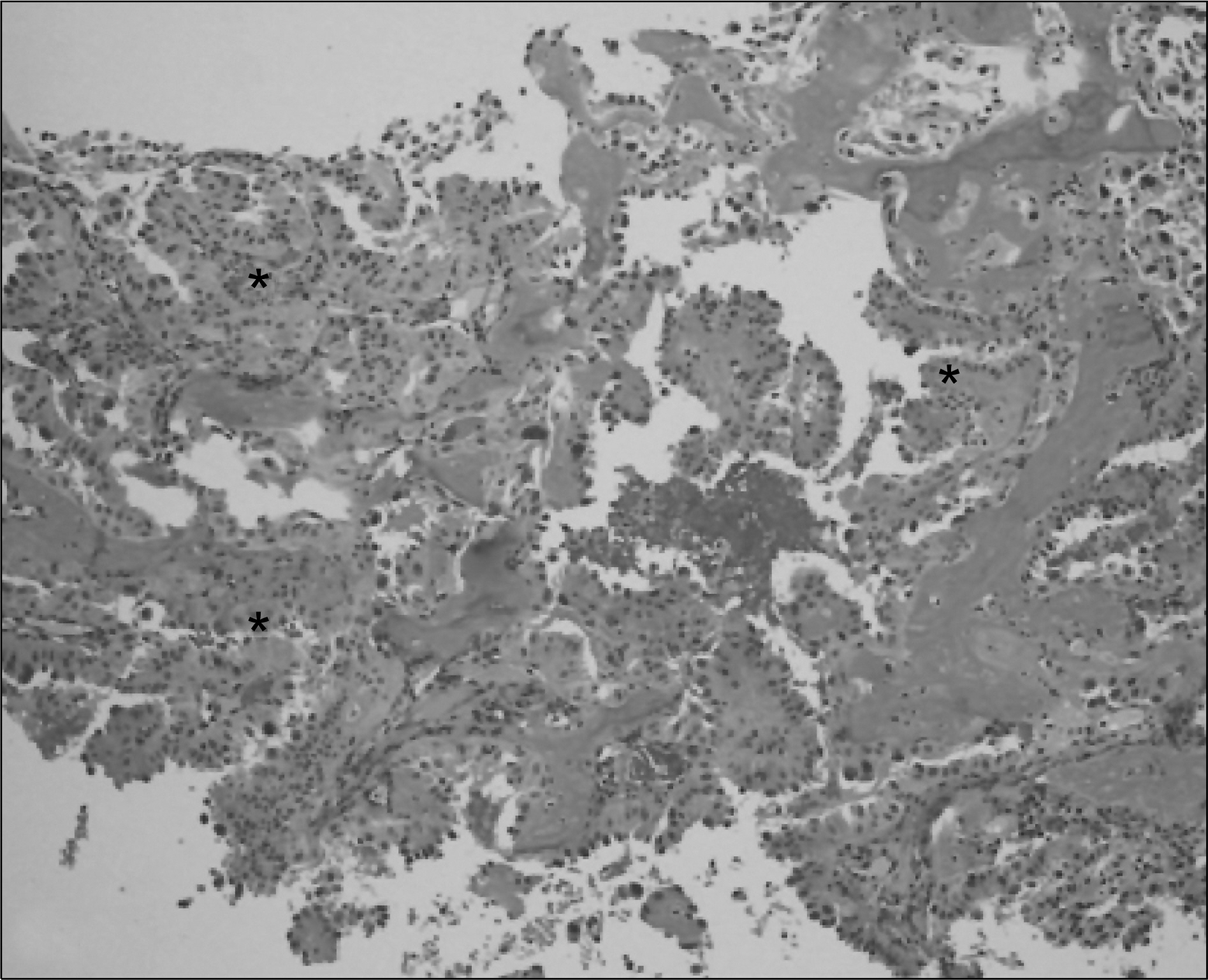
Fig. 4. Adenocarcinoma with subtle papillary pattern (asterisks) was noticed on H&E stain of core biopsied tissue (H&E, ×200).
Reference
-
References
1. Petrov D, Marchalik D, Lipsky A, Milgraum S. Asymptomatic enlargement of the clavicle: a review of underlying aetiologies. Acta Orthop Belg. 2010; 76:715–8.2. Robinson CM, Jenkins PJ, Markham PE, Beggs I. Disorders of the sternoclavicular joint. J Bone Joint Surg Br. 2008; 90:685–96.
Article3. Sugiura H, Yamada K, Sugiura T, Hida T, Mitsudomi T. Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop Relat Res. 2008; 466:729–36.
Article4. Dennis JL, Hvidsten TR, Wit EC, et al. Markers of adenocarcinoma characteristic of the site of origin: development of a diagnostic algorithm. Clin Cancer Res. 2005; 11:3766–72.
Article5. Welsh JW, Komaki R, Amini A, et al. Phase II trial of erlotinib plus concurrent whole-brain radiation therapy for patients with brain metastases from non-small-cell lung cancer. J Clin Oncol. 2013; 31:895–902.6. Sewell MD, Al-Hadithy N, Le Leu A, Lambert SM. Instability of the sternoclavicular joint: current concepts in classification, treatment and outcomes. Bone Joint J. 2013; 95:721–31.7. Shenoy R, Pillai A, Ried R, Tansey P. Primary bone tumors and tumor like lesions of the clavicle. Orthop proc. 2006; 88:297–8.8. Kapoor S, Tiwari A, Kapoor S. Primary tumours and tumorous lesions of clavicle. Int Orthop. 2008; 32:829–34.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Traumatic Posterior Dislocation of the Sternoclavicular Joint: A Case Report
- A Case of Metastatic Calcification Occurring at Sternoclavicular Joint in a Patient Receiving Maintenance Hemodialysis
- Traumatic Posterior Dislocation of the Sternoclavicular Joint: A case Report
- Treatment of Traumatic Sternoclavicular Joint Anterior Dislocation with a Sternal Fracture
- Posterior Sternoclavicular Dislocation: A Case Report
