J Korean Ophthalmol Soc.
2017 Apr;58(4):455-458. 10.3341/jkos.2017.58.4.455.
A Case of Fungal Ball Causing Acute Dacryocystitis
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. yswoph@hanmail.net
- KMID: 2376602
- DOI: http://doi.org/10.3341/jkos.2017.58.4.455
Abstract
- PURPOSE
We report a case of fungal ball after Endoscopic Dacryocystorhinostomy (DCR) in a 40-year-old female patient.
CASE SUMMARY
A 40-year-old female patient was admitted to our hospital for left lower eyelid tenderness and bloody discharge from the lacrimal punctum. During a planned endoscopic DCR, the sac was opened after the osteotomy, and 2 fungal balls were found in the lacrimal sac. The masses were 7 × 5 mm and, 9 × 5 mm sized, irregularly shaped, and red in color. Aspergillus fumigatus was diagnosed pathologically. Postoperative paranasal sinus magnetic resonance imaging showed no residual fungal ball. During follow-up, the patient showed patent rhinostomy opening, and there was no evidence of fungal infection on nasal endoscopic finding.
CONCLUSIONS
Although Aspergillus fumigatus is a rare cause of canalicular obstruction, fungal ball development in the lacrimal sac can cause acute dacryocystitis.
MeSH Terms
Figure
-

Figure 1. Gross finding of mass. 7 × 5 mm, 9 × 5 mm sized, ir-regularly shaped, red colored 2 fungal balls obstructing the lac-rimal sac.

Figure 2. Histologic finding of fungal ball (Periodic acid– Schiff stain, ×200). Numerous septated branched fungal hy-phae with degeneration and inflammatory cells, consistent with Aspergillosis.
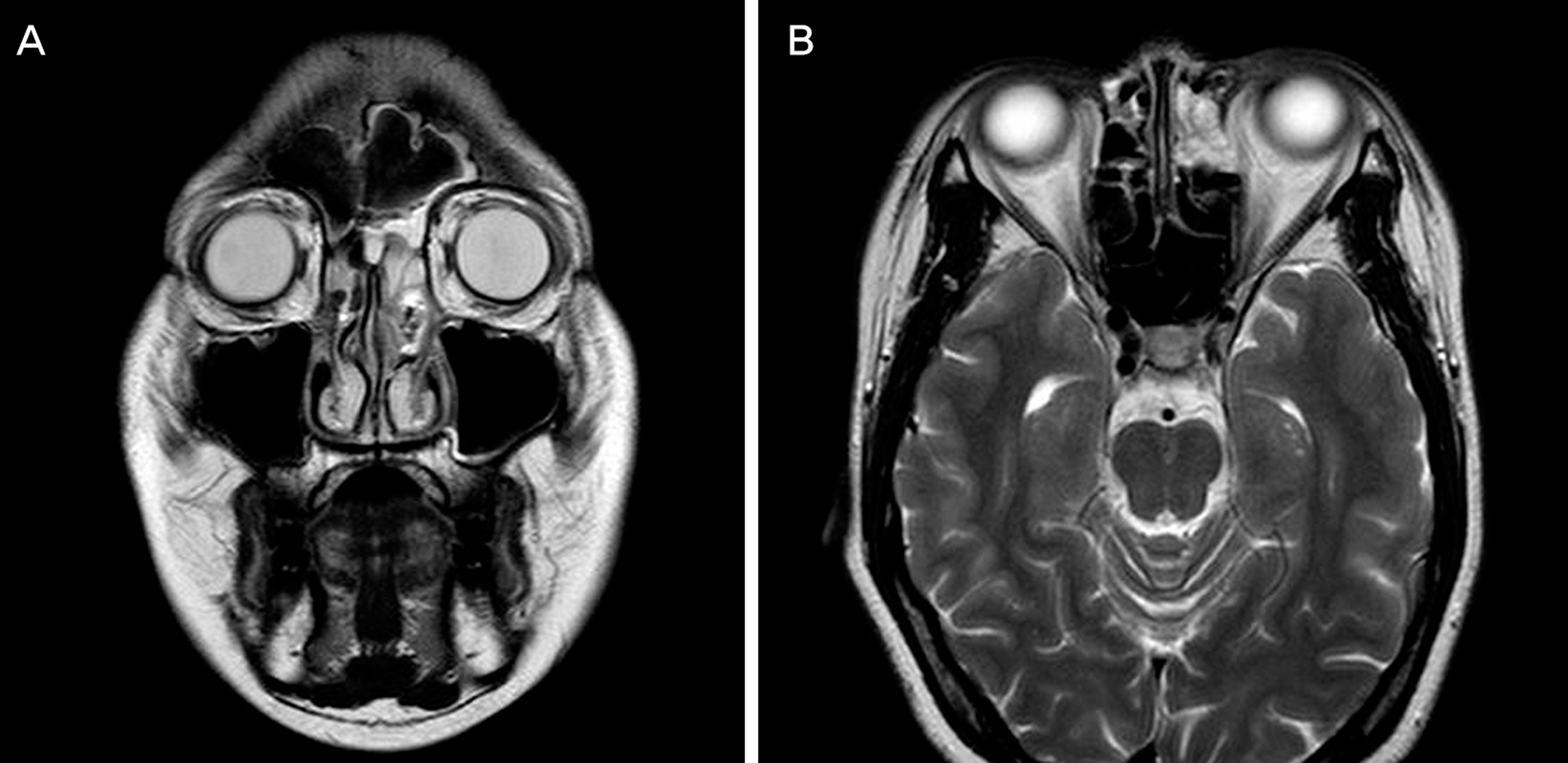
Figure 3. Paransal sinus magnetic resonance imaging (MRI), showing left ethmoid sinusitis. There is no remained visible fungal ball. (A) Coronal T2 MR image. (B) Axial T2 MR image.
Reference
-
References
1. Ali MJ, Joshi SD, Naik MN, Honavar SG. . Clinical profile and management outcome of acute dacryocystitis: two decades of experience in a tertiary eye care center. Semin Ophthalmol. 2015; 30:118–23.
Article2. Gregg KS, Kauffman CA. . Invasive Aspergillosis: epidemiology, clinical aspects, and treatment. Semin Respir Crit Care Med. 2015; 36:662–72.
Article3. Brightbill FS, Fraser LK. . Unilateral keratoconjunctivitis with ca-nalicular obstruction by Aspergillus fumigatus. Arch Ophthalmol. 1974; 91:421–2.4. Bartley GB. . Acquired lacrimal drainage obstruction: an etiologic classification system, case reports, and a review of the literature. Part 1. Ophthal Plast Reconstr Surg. 1992; 8:237–42.5. Obi E, Roy A, Bates V, Sandy C. . Bilateral chronic fungal dacryo-cystitis caused by Candida dubliniensis in a neutropenic patient. J Clin Pathol. 2006; 59:1194–5.
Article6. Davies BW, Gonzalez MO, Vaughn RC. . Dacryocystitis as the initial presentation of invasive fungal sinusitis in immunocompro-mised children. Ophthal Plast Reconstr Surg. 2016; 32:e79–81.
Article7. Kubo M, Sakuraba T, Wada R. . Clinicopathological features of da-cryolithiasis in Japanese patients: frequent association with in-fection in aged patients. ISRN Ophthalmol. 2013; 2013:406153.
Article8. Lim JW, Suh JW, Lee SJ. . A case of fungall ball after external dacryocystorhinostomy. J Korean Ophthalmol Soc. 2006; 47:1481–5.9. Han MS, Kim YH, Lee JH. . The fungal infection of nasal cavity af-ter endonasal dacryocystorhinostomy. J Korean Ophthalmol Soc. 2003; 44:1433–6.10. Cho HS, Lee KE, Kim KS. . Two cases of fungus ball in bilateral paranasal sinuses. Korean J Otorhinolaryngology-Head Neck Surg. 2014; 57:185–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Actinomycosis of the Maxillary Sinus Accompanied with Fungal Ball
- A Case of Fungal Ball with Cholesterol Granuloma in the Middle Ear Cavity
- Bacterial Urosepsis by a Fungal Ball Mimicking a Ureteral Stone
- A Case of Fungall Ball after External Dacryocystorhinostomy
- A Case of Fungal Ball Caused by Retained Glass Foreign Body in Maxillary Sinus for 30 Years
