Clinical Practice Patterns of Radiotherapy in Patients with Hepatocellular Carcinoma: A Korean Radiation Oncology Group Study (KROG 14-07)
- Affiliations
-
- 1Department of Radiation Oncology, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Korea. jsseong@yuhs.ac
- 2Department of Radiation Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Medical Device Management and Research, SAIHST, Sungkyunkwan University, Seoul, Korea.
- 4Research Institute and Hospital, National Cancer Center, Goyang, Korea.
- 5Department of Radiation Oncology, Chonnam National University Medical School, Gwangju, Korea.
- 6Department of Radiation Oncology, Asan Liver Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 7Department of Radiation Oncology, Korea University Ansan Hospital, Ansan, Korea.
- 8Department of Radiation Oncology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 9Department of Radiation Oncology, Korea Institute of Radiological and Medical Sciences, Seoul, Korea.
- 10Department of Radiation Oncology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 11Department of Radiation Oncology, Dong-A University College of Medicine, Busan, Korea.
- 12Department of Radiation Oncology, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea.
- 13Department of Radiation Oncology, Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Incheon, Korea.
- 14Department of Biostatistics, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2367504
- DOI: http://doi.org/10.4143/crt.2016.097
Abstract
- PURPOSE
The aim of this study was to examine patterns of radiotherapy (RT) in Korean patients with hepatocellular carcinoma (HCC) according to the evolving guideline for HCC established by the Korean Liver Cancer Study Group-National Cancer Center (KLCSG-NCC).
MATERIALS AND METHODS
We reviewed 765 patients with HCC who were treated with RT between January 2011 and December 2012 in 12 institutions.
RESULTS
The median follow-up period was 13.3 months (range, 0.2 to 51.7 months). Compared with previous data between 2004 and 2005, the use of RT as a first treatment has increased (9.0% vs. 40.8%). Increased application of intensity-modulated RT resulted in an increase in radiation dose (fractional dose, 1.8 Gy vs. 2.5 Gy; biologically effective dose, 53.1 Gy10 vs. 56.3 Gy10). Median overall survival was 16.2 months, which is longer than that reported in previous data (12 months). In subgroup analysis, treatments were significantly different according to stage (p < 0.001). Stereotactic body RT was used in patients with early HCC, and most patients with advanced stage were treated with three-dimensional conformal RT.
CONCLUSION
Based on the evolving KLCSG-NCC practice guideline for HCC, clinical practice patterns of RT have changed. Although RT is still used mainly in advanced HCC, the number of patients with good performance status who were treated with RT as a first treatment has increased. This change in practice patterns could result in improvement in overall survival.
MeSH Terms
Figure
-

Fig. 1. Overall survival. During the follow-up period, 455 patients died. Median overall survival for all patients was 16.2 months and the 2-year survival rate was 37.7%.

Fig. 2. (A) Pattern of failure. Assessment of treatment outcome was available in 734 patients (95.9%). Infield and outfield failure occurred in 235 (32.0%) and 547 (74.5%) patients. (B) Failure-free survival (FFS) for infield failure. Median FFS was not reached and 2-year FFS rate was 58.6%. (C) FFS for outfield failure. Median FFS was 9.8 months and 2-year FFS was 19.9%.
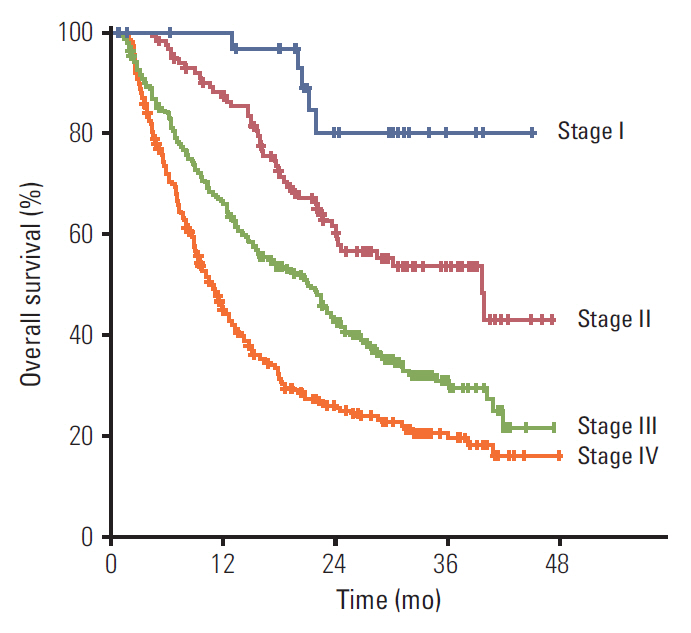
Fig. 3. Overall survival according to stage. Overall survival rates at 2 years in each stage were 76.7%, 60.4%, 42.9%, and 22.0%, respectively, and it was significantly different by stage (p < 0.001).
Cited by 3 articles
-
2018 Korean Liver Cancer Association–National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma
,
Korean J Radiol. 2019;20(7):1042-1113. doi: 10.3348/kjr.2019.0140.Treatment Outcome after Fractionated Conformal Radiotherapy for Hepatocellular Carcinoma in Patients with Child-Pugh Classification B in Korea (KROG 16-05)
Sun Hyun Bae, Hee Chul Park, Won Sup Yoon, Sang Min Yoon, In-Hye Jung, Ik Jae Lee, Jun Won Kim, Jinsil Seong, Tae Hyun Kim, Taek-Keun Nam, Youngmin Choi, Sun Young Lee, Hong Seok Jang, Dong Soo Lee, Jin Hee Kim
Cancer Res Treat. 2019;51(4):1589-1599. doi: 10.4143/crt.2018.687.2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma
J Liver Cancer. 2023;23(1):1-120. doi: 10.17998/jlc.2022.11.07.
Reference
-
References
1. Jung KW, Won YJ, Kong HJ, Oh CM, Cho H, Lee DH, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2012. Cancer Res Treat. 2015; 47:127–41.
Article2. Park JW; Korean Liver Cancer Study Group and National Cancer Center. Practice guideline for diagnosis and treatment of hepatocellular carcinoma. Korean J Hepatol. 2004; 10:88–98.3. Seong J, Lee IJ, Shim SJ, Lim DH, Kim TH, Kim JH, et al. A multicenter retrospective cohort study of practice patterns and clinical outcome on radiotherapy for hepatocellular carcinoma in Korea. Liver Int. 2009; 29:147–52.
Article4. Korean Liver Cancer Study Group and National Cancer Center. Practice guidelines for management of hepatocellular carcinoma 2009. Korean J Hepatol. 2009; 15:391–423.5. Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Dis. 2010; 30:61–74.
Article6. Dawson LA. Overview: where does radiation therapy fit in the spectrum of liver cancer local-regional therapies? Semin Radiat Oncol. 2011; 21:241–6.
Article7. Lee IJ, Seong J. Radiotherapeutic strategies in the management of hepatocellular carcinoma. Oncology. 2011; 81 Suppl 1:123–33.
Article8. Cha J, Seong J. Application of radiotherapeutic strategies in the BCLC-defined stages of hepatocellular carcinoma. Liver Cancer. 2012; 1:216–25.
Article9. Korean Liver Cancer Study Group (KLCSG); National Cancer Center, Korea (NCC). 2014 KLCSG-NCC Korea practice guideline for the management of hepatocellular carcinoma. Gut Liver. 2015; 9:267–317.10. Jang WI, Kim MS, Bae SH, Cho CK, Yoo HJ, Seo YS, et al. High-dose stereotactic body radiotherapy correlates increased local control and overall survival in patients with inoperable hepatocellular carcinoma. Radiat Oncol. 2013; 8:250.
Article11. Huertas A, Baumann AS, Saunier-Kubs F, Salleron J, Oldrini G, Croise-Laurent V, et al. Stereotactic body radiation therapy as an ablative treatment for inoperable hepatocellular carcinoma. Radiother Oncol. 2015; 115:211–6.
Article12. Bae SH, Kim MS, Jang WI, Kay CS, Kim W, Kim ES, et al. A survey of stereotactic body radiotherapy in Korea. Cancer Res Treat. 2015; 47:379–86.
Article13. Choi C, Koom WS, Kim TH, Yoon SM, Kim JH, Lee HS, et al. A prospective phase 2 multicenter study for the efficacy of radiation therapy following incomplete transarterial chemoembolization in unresectable hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2014; 90:1051–60.14. Cho JY, Paik YH, Park HC, Yu JI, Sohn W, Gwak GY, et al. The feasibility of combined transcatheter arterial chemoembolization and radiotherapy for advanced hepatocellular carcinoma. Liver Int. 2014; 34:795–801.
Article15. Shim SJ, Seong J, Han KH, Chon CY, Suh CO, Lee JT. Local radiotherapy as a complement to incomplete transcatheter arterial chemoembolization in locally advanced hepatocellular carcinoma. Liver Int. 2005; 25:1189–96.
Article16. Cha H, Yoon HI, Lee IJ, Koom WS, Han KH, Seong J. Clinical factors related to recurrence after hepatic arterial concurrent chemoradiotherapy for advanced but liver-confined hepatocellular carcinoma. J Radiat Res. 2013; 54:1069–77.
Article17. Choi Y, Kim JW, Cha H, Han KH, Seong J. Overall response of both intrahepatic tumor and portal vein tumor thrombosis is a good prognostic factor for hepatocellular carcinoma patients receiving concurrent chemoradiotherapy. J Radiat Res. 2014; 55:113–20.
Article18. Kang MK, Kim MS, Kim SK, Ye GW, Lee HJ, Kim TN, et al. High-dose radiotherapy with intensity-modulated radiation therapy for advanced hepatocellular carcinoma. Tumori. 2011; 97:724–31.
Article19. Yoon HI, Lee IJ, Han KH, Seong J. Improved oncologic outcomes with image-guided intensity-modulated radiation therapy using helical tomotherapy in locally advanced hepatocellular carcinoma. J Cancer Res Clin Oncol. 2014; 140:1595–605.
Article20. Kim TH, Park JW, Kim YJ, Kim BH, Woo SM, Moon SH, et al. Simultaneous integrated boost-intensity modulated radiation therapy for inoperable hepatocellular carcinoma. Strahlenther Onkol. 2014; 190:882–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Application of radiotherapy for hepatocellular carcinoma in current clinical practice guidelines
- Recent developments in radiotherapy for hepatocellular carcinoma
- Differences in radiotherapy application according to regional disease characteristics of hepatocellular carcinoma
- Current status of stereotactic body radiotherapy for the treatment of hepatocellular carcinoma
- Novel paradigm in the treatment of hepatocellular carcinoma: Anticipating breakthroughs with particle therapy
