Arthroscopic Bioabsorbable Screw Fixation of Unstable Osteochondritis Dissecans in Adolescents: Clinical Results, Magnetic Resonance Imaging, and Second-Look Arthroscopic Findings
- Affiliations
-
- 1Department of Orthopedic Surgery, Pohang Naval Hospital, Pohang, Korea.
- 2Department of Orthopaedic Surgery, Wonkwang University Hospital, Wonkwang University School of Medicine, Iksan, Korea. cch@wonkwang.ac.kr
- 3Institutue of Wonkwang Medical Science, Iksan, Korea.
- KMID: 2363946
- DOI: http://doi.org/10.4055/cios.2016.8.1.57
Abstract
- BACKGROUND
This study aimed to evaluate the clinical and radiological outcomes of arthroscopic bioabsorbable screw fixation in osteochondritis dissecans (OCD) in adolescent patients with unstable lesions causing pain.
METHODS
The study included 11 patients (10 males and 1 female) with OCD who underwent arthroscopic bioabsorbable screw fixation between July 2007 and February 2014 and were available for follow-up for more than 12 months. The mean age at diagnosis was 16.3 years (range, 11 to 19 years), and the average follow-up period was 51 months (range, 12 to 91 months). Clinical results were evaluated using the Knee Injury and Osteoarthritis Outcome Score (KOOS), Lysholm knee score, and International Knee Documentation Committee (IKDC) score measured before surgery and at follow-up. Functional evaluation was made using the Tegner activity scale. Magnetic resonance imaging (MRI) and second-look arthroscopy were performed at the 12-month follow-up.
RESULTS
Between the preoperative assessment and follow-up, improvements were seen in the KOOS (range, 44.9 to 88.1), Lysholm knee score (range, 32.6 to 82.8), and IKDC score (range, 40.8 to 85.6). The Tegner activity scale also improved from 2.8 to 6.1. Based on postoperative MRI, there were eight Dipaola grade I cases and three grade II cases. No complications due to fixation failure developed in any case. Second-look arthroscopy at 12 months postoperatively revealed that the lesion was covered with cartilage in all cases.
CONCLUSIONS
For unstable OCD lesions causing pain in adolescents, arthroscopic bioabsorbable screw fixation provided favorable outcomes with reduced pain and restoration of movement. Therefore, it should be considered as an effective treatment for OCD.
MeSH Terms
Figure
-
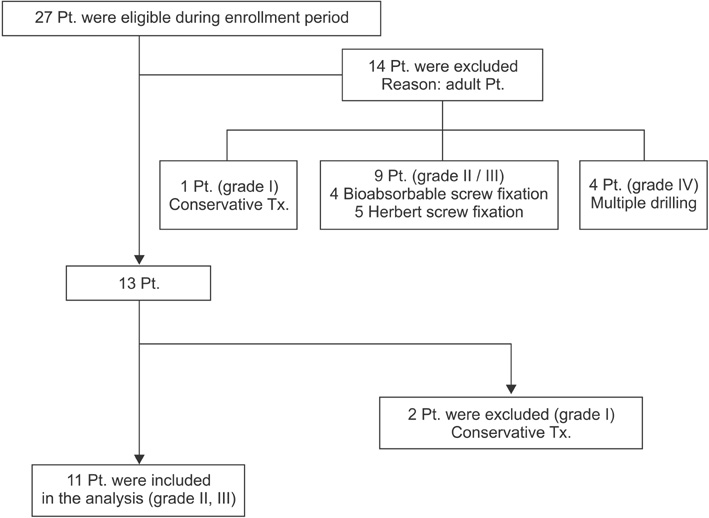
Fig. 1 Study participant flow chart. Pt.: patients, Tx.: treatment.
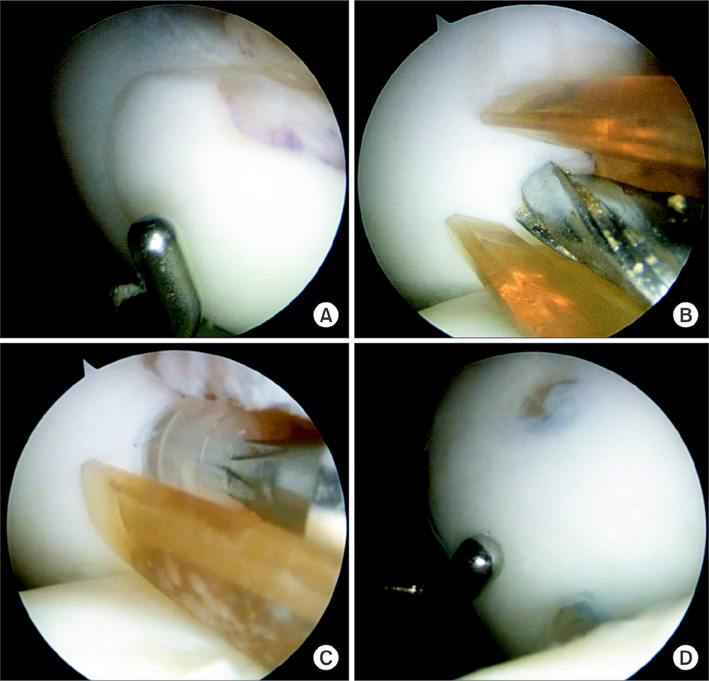
Fig. 2 (A) The arthroscopic image from case no.2 shows an unstable lesion of the medial femoral condyle. (B) The drill guide is inserted in the vertical position into the lesion. (C) A bioabsorbable screw is inserted with vertical compression force. (D) The arthroscopic image shows three bioabsorbable screws in the osteochondritis dissecans lesion.
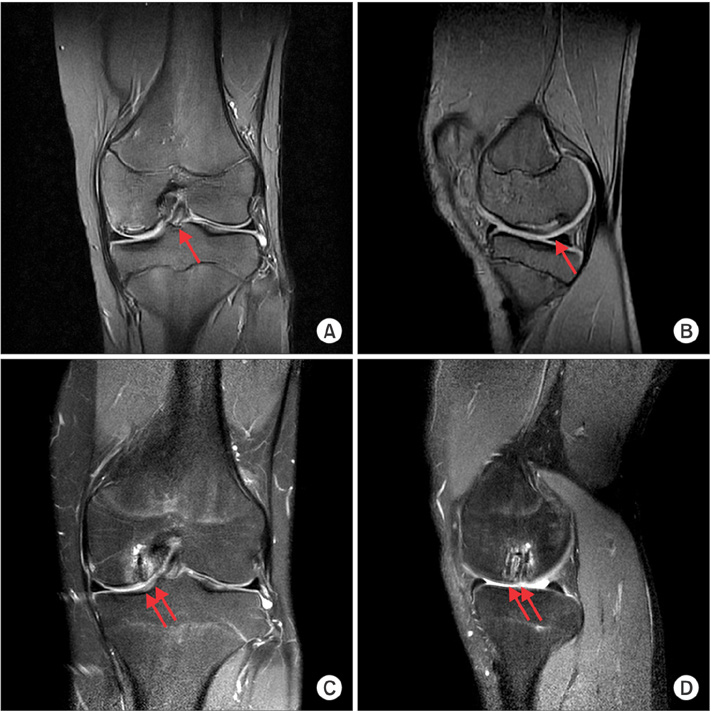
Fig. 3 (A, B) The preoperative magnetic resonance imaging (T2 fat suppression) scans from case no.2 show osteochondritis dissecans of the medial femoral condyle (arrow). (C, D) The magnetic resonance imaging scans taken at follow-up, 12 months after operation, show three bioabsorbable screws (arrows) fixed with nearly normal congruency of the articular surface overlying the fixation site.
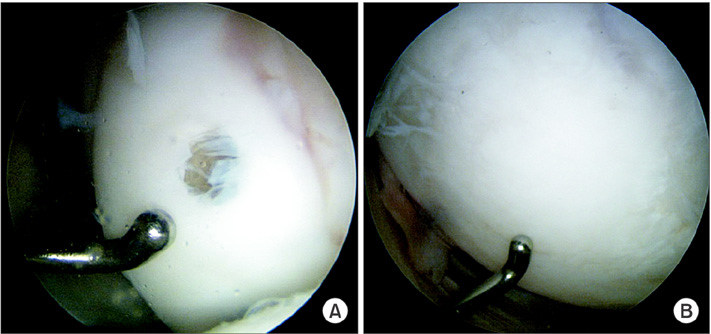
Fig. 4 (A) The preoperative arthroscopic image shows bioabsorbable screw fixation of the osteochondritis dissecans lesion. (B) The second-look arthroscopy image at 12 months postoperatively revealed that the lesion is covered with cartilage.
Reference
-
1. Cahill BR. Osteochondritis dissecans of the knee: treatment of juvenile and adult forms. J Am Acad Orthop Surg. 1995; 3(4):237–247.
Article2. Sales de Gauzy J, Mansat C, Darodes PH, Cahuzac JP. Natural course of osteochondritis dissecans in children. J Pediatr Orthop B. 1999; 8(1):26–28.
Article3. Linden B. Osteochondritis dissecans of the femoral condyles: a long-term follow-up study. J Bone Joint Surg Am. 1977; 59(6):769–776.4. Jakob RP, Franz T, Gautier E, Mainil-Varlet P. Autologous osteochondral grafting in the knee: indication, results, and reflections. Clin Orthop Relat Res. 2002; (401):170–184.
Article5. Prakash D, Learmonth D. Natural progression of osteo-chondral defect in the femoral condyle. Knee. 2002; 9(1):7–10.
Article6. Cain EL, Clancy WG. Treatment algorithm for osteochondral injuries of the knee. Clin Sports Med. 2001; 20(2):321–342.
Article7. Kivisto R, Pasanen L, Leppilahti J, Jalovaara P. Arthroscopic repair of osteochondritis dissecans of the femoral condyles with metal staple fixation: a report of 28 cases. Knee Surg Sports Traumatol Arthrosc. 2002; 10(5):305–309.
Article8. Lipscomb PR Jr, Lipscomb PR Sr, Bryan RS. Osteochondritis dissecans of the knee with loose fragments: treatment by replacement and fixation with readily removed pins. J Bone Joint Surg Am. 1978; 60(2):235–240.
Article9. Dervin GF, Keene GC, Chissell HR. Biodegradable rods in adult osteochondritis dissecans of the knee. Clin Orthop Relat Res. 1998; (356):213–221.
Article10. Kocher MS, Tucker R, Ganley TJ, Flynn JM. Management of osteochondritis dissecans of the knee: current concepts review. Am J Sports Med. 2006; 34(7):1181–1191.
Article11. Murray JR, Chitnavis J, Dixon P, et al. Osteochondritis dissecans of the knee; long-term clinical outcome following arthroscopic debridement. Knee. 2007; 14(2):94–98.
Article12. Dipaola JD, Nelson DW, Colville MR. Characterizing osteochondral lesions by magnetic resonance imaging. Arthroscopy. 1991; 7(1):101–104.
Article13. Guhl JF. Arthroscopic treatment of osteochondritis dissecans. Clin Orthop Relat Res. 1982; (167):65–74.
Article14. Hughston JC, Hergenroeder PT, Courtenay BG. Osteochondritis dissecans of the femoral condyles. J Bone Joint Surg Am. 1984; 66(9):1340–1348.
Article15. Twyman RS, Desai K, Aichroth PM. Osteochondritis dissecans of the knee: a long-term study. J Bone Joint Surg Br. 1991; 73(3):461–464.
Article16. Cepero S, Ullot R, Sastre S. Osteochondritis of the femoral condyles in children and adolescents: our experience over the last 28 years. J Pediatr Orthop B. 2005; 14(1):24–29.
Article17. Aglietti P, Buzzi R, Bassi PB, Fioriti M. Arthroscopic drilling in juvenile osteochondritis dissecans of the medial femoral condyle. Arthroscopy. 1994; 10(3):286–291.
Article18. Kocher MS, Micheli LJ, Yaniv M, Zurakowski D, Ames A, Adrignolo AA. Functional and radiographic outcome of juvenile osteochondritis dissecans of the knee treated with transarticular arthroscopic drilling. Am J Sports Med. 2001; 29(5):562–566.
Article19. Kouzelis A, Plessas S, Papadopoulos AX, Gliatis I, Lambiris E. Herbert screw fixation and reverse guided drillings, for treatment of types III and IV osteochondritis dissecans. Knee Surg Sports Traumatol Arthrosc. 2006; 14(1):70–75.
Article20. Fonseca F, Balaco I. Fixation with autogenous osteochondral grafts for the treatment of osteochondritis dissecans (stages III and IV). Int Orthop. 2009; 33(1):139–144.
Article21. Kobayashi T, Fujikawa K, Oohashi M. Surgical fixation of massive osteochondritis dissecans lesion using cylindrical osteochondral plugs. Arthroscopy. 2004; 20(9):981–986.
Article22. Miura K, Ishibashi Y, Tsuda E, Sato H, Toh S. Results of arthroscopic fixation of osteochondritis dissecans lesion of the knee with cylindrical autogenous osteochondral plugs. Am J Sports Med. 2007; 35(2):216–222.
Article23. Gudas R, Simonaityte R, Cekanauskas E, Tamosiunas R. A prospective, randomized clinical study of osteochondral autologous transplantation versus microfracture for the treatment of osteochondritis dissecans in the knee joint in children. J Pediatr Orthop. 2009; 29(7):741–748.
Article24. Din R, Annear P, Scaddan J. Internal fixation of undisplaced lesions of osteochondritis dissecans in the knee. J Bone Joint Surg Br. 2006; 88(7):900–904.
Article25. Larsen MW, Pietrzak WS, DeLee JC. Fixation of osteochondritis dissecans lesions using poly(l-lactic acid)/ poly(glycolic acid) copolymer bioabsorbable screws. Am J Sports Med. 2005; 33(1):68–76.
Article26. Scioscia TN, Giffin JR, Allen CR, Harner CD. Potential complication of bioabsorbable screw fixation for osteochondritis dissecans of the knee. Arthroscopy. 2001; 17(2):E7.
Article27. Millington KL, Shah JP, Dahm DL, Levy BA, Stuart MJ. Bioabsorbable fixation of unstable osteochondritis dissecans lesions. Am J Sports Med. 2010; 38(10):2065–2070.
Article28. Webb JE, Lewallen LW, Christophersen C, Krych AJ, Mc-Intosh AL. Clinical outcome of internal fixation of unstable juvenile osteochondritis dissecans lesions of the knee. Orthopedics. 2013; 36(11):e1444–e1449.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fixation Method Using Bioabsorbable Pins for Osteochondritis Dissecans in the Knee through Mini-Open Approach
- Arthroscopic herbert screw fixation in osteochondritis dissecans ofof the knee
- Osteochondritis Dissecans of the Knee
- Arthroscopic surgical treatment of osteochondritis dissecans of theknee
- Outcomes of Operative Management of Juvenile Osteochondritis Dissecans of the Knee in Athletes
