Korean J Neurotrauma.
2016 Oct;12(2):77-83. 10.13004/kjnt.2016.12.2.77.
Biomarkers of Physiological Disturbances for Predicting Mortality in Decompressive Craniectomy
- Affiliations
-
- 1Department of Neurosurgery, Wonju Severance Christian Hospital, Yonsei University, Wonju, Korea. whangkum@yonsei.ac.kr
- 2Institute of Lifestyle Medicine, Wonju College of Medicine, Yonsei University, Wonju, Korea.
- KMID: 2356777
- DOI: http://doi.org/10.13004/kjnt.2016.12.2.77
Abstract
OBJECTIVE
Of many critical care regimens, the management of physiological disturbances in serum is particularly drawing an attention in conjunction with patient outcome. The aim of this study was to assess the association of serum biochemical markers with mortality in head trauma patients with decompressive craniotomy.
METHODS
Ninety six patients with acute subdural hematoma underwent decompressive craniectomy between January 2014 and December 2015. The clinical data and laboratory variables of these patients were recorded and analyzed retrospectively. The pre-operative and post-operative day (POD) 0, day 1 and day 2 serum variables were measured. These were compared between the survivors and non-survivors.
RESULTS
The factors of a large amount of intra-operative blood loss, shorter length of intensive care unit stays, and the needs for mechanical ventilation were related with mortality in the patients with decompressive craniectomy. These clinical factors were associated with the physiological derangements of sera. The average difference in serum chloride concentration between the pre-operative and POD 2 measurements (p=0.0192) showed a statistical significance in distinguishing between survivors and non-survivors. The average differences in albumin (p=0.0011) and platelet count (p=0.0004) between the pre-operative and POD 0 measurements suggested to be strong predictors of mortality in decompressive craniectomy.
CONCLUSION
Isolated values of physiological biomarkers are not sufficient enough to predict in-hospital mortality. This study emphasizes the importance of a combined prognostic model of the differences in the pre-operative and post-operative hyperchloremia, thrombocytopenia, and hypoalbuminemia to identify the risk of mortality in decompressive craniecomy.
MeSH Terms
Figure
-
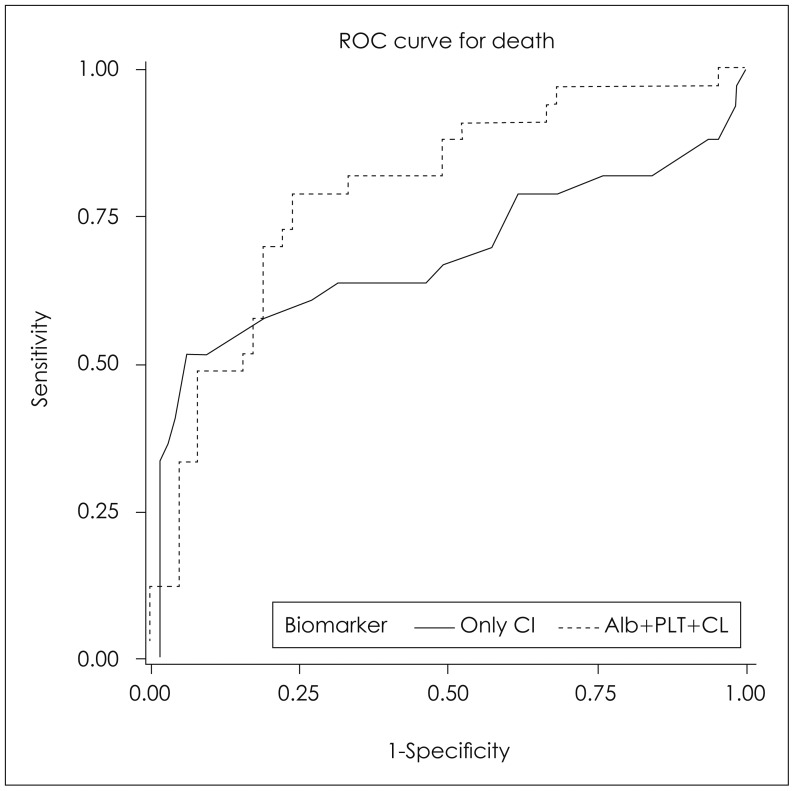
FIGURE 1 Receiver operating characteristic curves for the model including chloride only (48 hours after surgery) and for the model including chloride (48 hours after surgery), albumin and platelet counts for in-hospital mortality. Areas under receiver-operating characteristic curve for chloride only was 0.683 and for including chloride (48 hours after surgery), albumin and platelet counts was 0.793 (p=0.0890). ROC: receiver-operating characteristic, CI: confidence interval, Alb: albumin, PLT: platelets, CL: chloride.
Reference
-
1. Allard CB, Scarpelini S, Rhind SG, Baker AJ, Shek PN, Tien H, et al. Abnormal coagulation tests are associated with progression of traumatic intracranial hemorrhage. J Trauma. 2009; 67:959–967. PMID: 19901655.
Article2. Baron DM, Hochrieser H, Metnitz PG, Mauritz W. Tracheostomy is associated with decreased hospital mortality after moderate or severe isolated traumatic brain injury. Wien Klin Wochenschr. 2016; 128:397–403. PMID: 27220338.
Article3. Bederson JB, Connolly ES Jr, Batjer HH, Dacey RG, Dion JE, Diringer MN, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 2009; 40:994–1025. PMID: 19164800.
Article4. Berend K, van Hulsteijn LH, Gans RO. Chloride: the queen of electrolytes? Eur J Intern Med. 2012; 23:203–211. PMID: 22385875.
Article5. Bratton SL, Chestnut RM, Ghajar J, McConnell Hammond FF, Harris OA, Hartl R, et al. Guidelines for the management of severe traumatic brain injury. II. Hyperosmolar therapy. J Neurotrauma. 2007; 24(Suppl 1):S14–S20. PMID: 17511539.6. Briggs A, Gates JD, Kaufman RM, Calahan C, Gormley WB, Havens JM. Platelet dysfunction and platelet transfusion in traumatic brain injury. J Surg Res. 2015; 193:802–806. PMID: 25218281.
Article7. Chibbaro S, Tacconi L. Role of decompressive craniectomy in the management of severe head injury with refractory cerebral edema and intractable intracranial pressure. Our experience with 48 cases. Surg Neurol. 2007; 68:632–638. PMID: 17765952.
Article8. de Gans K, de Haan RJ, Majoie CB, Koopman MM, Brand A, Dijkgraaf MG, et al. PATCH: platelet transfusion in cerebral haemorrhage: study protocol for a multicentre, randomised, controlled trial. BMC Neurol. 2010; 10:19. PMID: 20298539.
Article9. Fencl V, Jabor A, Kazda A, Figge J. Diagnosis of metabolic acid-base disturbances in critically ill patients. Am J Respir Crit Care Med. 2000; 162:2246–2251. PMID: 11112147.
Article10. Finfer S, Bellomo R, Boyce N, French J, Myburgh J, Norton R. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med. 2004; 350:2247–2256. PMID: 15163774.
Article11. Gantner D, Moore EM, Cooper DJ. Intravenous fluids in traumatic brain injury: what's the solution? Curr Opin Crit Care. 2014; 20:385–389. PMID: 24979716.12. Hucker TR, Mitchell GP, Blake LD, Cheek E, Bewick V, Grocutt M, et al. Identifying the sick: can biochemical measurements be used to aid decision making on presentation to the accident and emergency department. Br J Anaesth. 2005; 94:735–741. PMID: 15805142.
Article13. Kaplan LJ, Kellum JA. Initial pH, base deficit, lactate, anion gap, strong ion difference, and strong ion gap predict outcome from major vascular injury. Crit Care Med. 2004; 32:1120–1124. PMID: 15190960.
Article14. Kunze E, Meixensberger J, Janka M, Sörensen N, Roosen K. Decompressive craniectomy in patients with uncontrollable intracranial hypertension. Acta Neurochir Suppl. 1998; 71:16–18. PMID: 9779131.
Article15. Maegele M. Coagulopathy after traumatic brain injury: incidence, pathogenesis, and treatment options. Transfusion. 2013; 53(Suppl 1):28s–37s. PMID: 23301970.
Article16. Maegele M, Schöchl H, Cohen MJ. An update on the coagulopathy of trauma. Shock. 2014; 41(Suppl 1):21–25. PMID: 24192549.
Article17. Martin M, Conlon LW. Does platelet transfusion improve outcomes in patients with spontaneous or traumatic intracerebral hemorrhage? Ann Emerg Med. 2013; 61:58–61. PMID: 22841709.
Article18. Moritz ML, Ayus JC. Water water everywhere: standardizing postoperative fluid therapy with 0.9% normal saline. Anesth Analg. 2010; 110:293–295. PMID: 20081126.
Article19. Nakamura N, Yamaura A, Shigemori M, Ono J, Kawamata T, Sakamoto T. Epidemiology, prevention and countermeasures against severe traumatic brain injury in Japan and abroad. Neurol Res. 2002; 24:45–53. PMID: 11783753.
Article20. Nicholson JP, Wolmarans MR, Park GR. The role of albumin in critical illness. Br J Anaesth. 2000; 85:599–610. PMID: 11064620.
Article21. Scheingraber S, Rehm M, Sehmisch C, Finsterer U. Rapid saline infusion produces hyperchloremic acidosis in patients undergoing gynecologic surgery. Anesthesiology. 1999; 90:1265–1270. PMID: 10319771.
Article22. Schnüriger B, Inaba K, Abdelsayed GA, Lustenberger T, Eberle BM, Barmparas G, et al. The impact of platelets on the progression of traumatic intracranial hemorrhage. J Trauma. 2010; 68:881–885. PMID: 20386283.
Article23. Shaw AD, Bagshaw SM, Goldstein SL, Scherer LA, Duan M, Schermer CR, et al. Major complications, mortality, and resource utilization after open abdominal surgery: 0.9% saline compared to Plasma-Lyte. Ann Surg. 2012; 255:821–829. PMID: 22470070.24. Silva Junior JM, Neves EF, Santana TC, Ferreira UP, Marti YN, Silva JM. The importance of intraoperative hyperchloremia. Rev Bras Anestesiol. 2009; 59:304–313. PMID: 19488543.25. Smith I, Kumar P, Molloy S, Rhodes A, Newman PJ, Grounds RM, et al. Base excess and lactate as prognostic indicators for patients admitted to intensive care. Intensive Care Med. 2001; 27:74–83. PMID: 11280677.
Article26. Van Aken HK, Kampmeier TG, Ertmer C, Westphal M. Fluid resuscitation in patients with traumatic brain injury: what is a SAFE approach? Curr Opin Anaesthesiol. 2012; 25:563–565. PMID: 22825048.27. Waldau T, Larsen VH, Bonde J, Fogh-Andersen N. Lactate, pH, and blood gas analysis in critically ill patients. Acta Anaesthesiol Scand Suppl. 1995; 107:267–271. PMID: 8599289.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The relationship between the serum lactate level and in-hospital mortality after decompressive craniectomy in traumatic brain Injury
- Paradoxical Herniation after Decompressive Craniectomy for Acute Subdural Hematoma
- Effects of Decompressive Craniectomy for the Management of Patients with Refractory Intracranial Hypertension
- Glasgow Coma Scale Motor Score Predicts Need for Tracheostomy After Decompressive Craniectomy for Traumatic Brain Injury
- The Effectiveness of Decompressive Craniectomy with Dural Augmentation in Malignant Cerebral Infarction
