Surgical Outcome of Adult Idiopathic Chiari Malformation Type 1
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea. chungc@snu.ac.kr
- 2Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea.
- 3Neuroscience Research Institute, Seoul National University Medical Research Center, Seoul, Korea.
- 4Clinical Research Institute, Seoul National University Hospital, Seoul, Korea.
- 5Department of Brain and Cognitive Sciences, Seoul National University College of Natural Sciences, Seoul, Korea.
- 6Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- 7Department of Neurosurgery, Seoul National University Boramae Hospital, Seoul, Korea.
- KMID: 2351721
- DOI: http://doi.org/10.3340/jkns.2016.59.5.512
Abstract
OBJECTIVE
The pathophysiology of idiopathic Chiari malformation (CM) type 1 is disturbance of free cerebrospinal fluid (CSF) flow and restoration of normal CSF flow is the mainstay of treatment. Additional migration of the medulla oblongata in pediatric patients is referred to as CM type 1.5, but its significance in adult patients is unknown. This study is to compare surgical outcomes of adult idiopathic CM type 1.5 with that of type 1.
METHODS
Thirty-eight consecutive adult patients (M : F=11 : 27; median, 33.5; range, 18-63) with syringomyelia due to idiopathic CM type 1 were reviewed. Migration of the medulla oblongata was noted in 13 patients. The modified McCormick scale (MMS) was used to evaluate functional status before and one year after surgery. All patients underwent foramen magnum decompression and duroplasty. Factors related to radiological success (≥50% decrease in the diameter of the syrinx) were investigated. The follow-up period was 72.7±55.6 months.
RESULTS
Preoperative functional status were MMS I in 11 patients and MMS II in 14 of CM type 1 and MMS I in 8 and II in 5 of CM type 1.5. Of patients with MMS II, 5/14 patients in group A and 3/5 patients in group B showed improvement and there was no case of deterioration. Radiological success was achieved in 32 (84%) patients and restoration of the cisterna magna (p=0.01; OR, 46.5) was the only significant factor.
CONCLUSION
Migration of the medulla oblongata did not make a difference in the surgical outcome when the cisterna magna was restored.
MeSH Terms
Figure
-
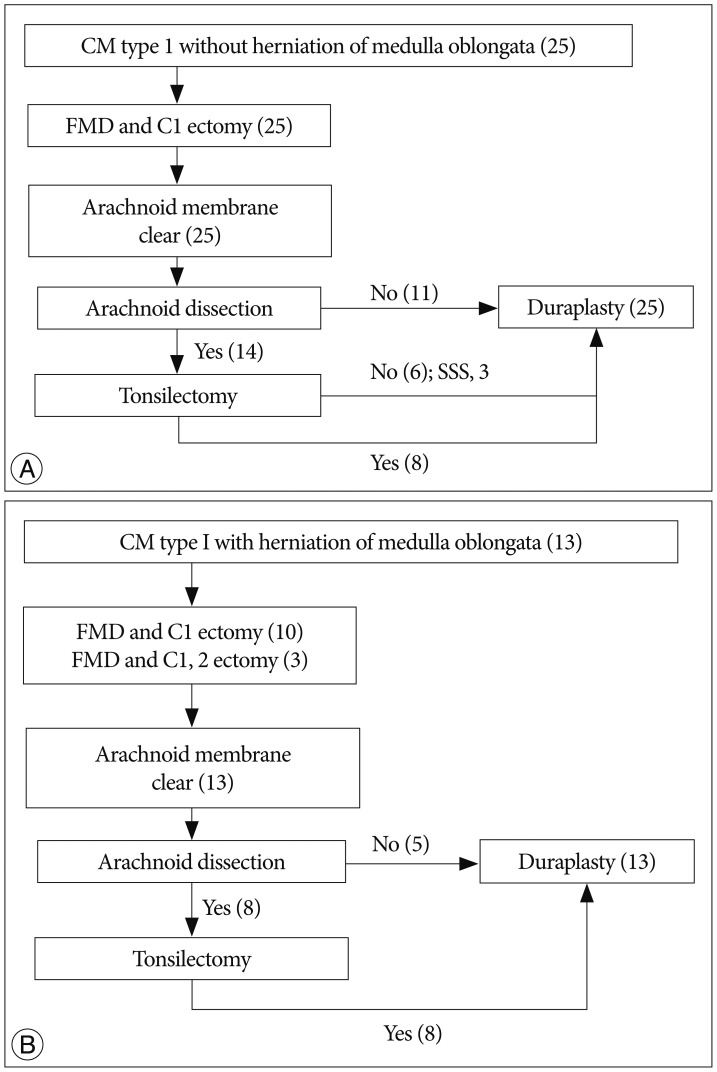
Fig. 1 The algorithm of the surgical procedures. The surgical procedures for Chiari malformation (CM) type 1 without herniation of the medulla oblongata (A). The numbers in parentheses represent the numbers of patients. Similarly, the surgical procedures for Chiari malformation type 1 with herniation of the medulla oblongata (B). FMD : foramen magnum decompression, C1 ectomy : removal of the posterior C1 ring, C2 ectomy : partial or total laminectomy of C2, SSS : syringo-subarachnoid shunt.

Fig. 2 Normalization of hindbrain herniation after restoration of the cisterna magna. The T2-weighted sagittal magnetic resonance (MR) image shows syringomyelia in the whole spine. The obex (arrow) and tonsil (double arrow) are located 16.1 mm and 17.2 mm, respectively, below the foramen magnum (A). Tonsillar beaking is observed. Postoperative day 2 : the syringomyelia is slightly reduced, but the retrocerebellar and subtonsillar subarachnoid spaces are not markedly changed (B). Postoperative month 6 : the syringomyelia is reduced by more than 50%, and restoration of the cisterna magna (*) is prominent (C). The length of the dorsal cerebrospinal fluid pathway is 14.5 mm. The tonsil and obex are located above the foramen magnum, and rounding of the tonsil is present.

Fig. 3 Aggravation of hindbrain herniation after failed restoration of the cisterna magna. The T2-weighted sagittal magnetic resonance (MR) image shows syringomyelia in the cervical and thoracic spine. The tonsil and obex are located 6.5 mm and 5.7 mm, respectively, below the foramen magnum (A). Tonsillar beaking is also present. Postoperative month 3 : the syringomyelia and hindbrain herniation are similar (B). The cisterna magna is not reconstructed. Postoperative month 50 : the obex lies 12.9 mm below the foramen magnum, with persistent syringomyelia (C).
Reference
-
1. Alfieri A, Pinna G. Long-term results after posterior fossa decompression in syringomyelia with adult Chiari Type I malformation. J Neurosurg Spine. 2012; 17:381–387. PMID: 22938552.
Article2. Bao C, Yang F, Liu L, Wang B, Li D, Gu Y, et al. Surgical treatment of Chiari I malformation complicated with syringomyelia. Exp Ther Med. 2013; 5:333–337. PMID: 23251294.
Article3. Batzdorf U, McArthur DL, Bentson JR. Surgical treatment of Chiari malformation with and without syringomyelia : experience with 177 adult patients. J Neurosurg. 2013; 118:232–242. PMID: 23176335.
Article4. Greitz D. Unraveling the riddle of syringomyelia. Neurosurg Rev. 2006; 29:251–263. discussion 264. PMID: 16752160.
Article5. Heiss JD, Suffredini G, Bakhtian KD, Sarntinoranont M, Oldfield EH. Normalization of hindbrain morphology after decompression of Chiari malformation Type I. J Neurosurg. 2012; 117:942–946. PMID: 22978540.
Article6. Kalb S, Perez-Orribo L, Mahan M, Theodore N, Nakaji P, Bristol RE. Evaluation of operative procedures for symptomatic outcome after decompression surgery for Chiari type I malformation. J Clin Neurosci. 2012; 19:1268–1272. PMID: 22771142.
Article7. Kim IK, Wang KC, Kim IO, Cho BK. Chiari 1.5 malformation : an advanced form of Chiari I malformation. J Korean Neurosurg Soc. 2010; 48:375–379. PMID: 21113370.
Article8. Kim J, Kim CH, Jahng TA, Chung CK. Clinical course of incidental syringomyelia without predisposing pathologies. J Clin Neurosci. 2012; 19:665–668. PMID: 22386658.
Article9. Klekamp J. Neurological deterioration after foramen magnum decompression for Chiari malformation type I : old or new pathology? J Neurosurg Pediatr. 2012; 10:538–547. PMID: 23039841.
Article10. Klekamp J. Surgical treatment of Chiari I malformation--analysis of intraoperative findings, complications, and outcome for 371 foramen magnum decompressions. Neurosurgery. 2012; 71:365–380. discussion 380. PMID: 22569058.
Article11. Klekamp J. The pathophysiology of syringomyelia - historical overview and current concept. Acta Neurochir (Wien). 2002; 144:649–664. PMID: 12181698.12. Koyanagi I, Houkin K. Pathogenesis of syringomyelia associated with Chiari type 1 malformation : review of evidences and proposal of a new hypothesis. Neurosurg Rev. 2010; 33:271–284. discussion 284-285. PMID: 20532585.
Article13. Lee JH, Chung CK, Kim HJ. Cerebral dissection from syringomyelia demonstrated using cine magnetic resonance imaging. Case report. J Neurosurg. 2001; 94:318–321. PMID: 11213972.
Article14. Lee JH, Chung CK, Kim HJ. Decompression of the spinal subarachnoid space as a solution for syringomyelia without Chiari malformation. Spinal Cord. 2002; 40:501–506. PMID: 12235531.
Article15. Logue V, Edwards MR. Syringomyelia and its surgical treatment--an analysis of 75 patients. J Neurol Neurosurg Psychiatry. 1981; 44:273–284. PMID: 7241155.
Article16. Loukas M, Noordeh N, Shoja MM, Pugh J, Oakes WJ, Tubbs RS. Hans Chiari (1851-1916). Childs Nerv Syst. 2008; 24:407–409. PMID: 18066558.
Article17. McCormick PC, Torres R, Post KD, Stein BM. Intramedullary ependymoma of the spinal cord. J Neurosurg. 1990; 72:523–532. PMID: 2319309.
Article18. Shamji MF, Ventureyra EC, Baronia B, Nzau M, Vassilyadi M. Classification of symptomatic Chiari I malformation to guide surgical strategy. Can J Neurol Sci. 2010; 37:482–487. PMID: 20724256.
Article19. Sohn S, Chung CK, Kim CH. Is closed-suction drainage necessary after intradural primary spinal cord tumor surgery? Eur Spine J. 2013; 22:577–583. PMID: 23001449.
Article20. Song SW, Chung CK. Acquired Chiari malformation. J Korean Neurosurg Soc. 2006; 40:38–39.21. Tubbs RS, Beckman J, Naftel RP, Chern JJ, Wellons JC 3rd, Rozzelle CJ, et al. Institutional experience with 500 cases of surgically treated pediatric Chiari malformation Type I. J Neurosurg Pediatr. 2011; 7:248–256. PMID: 21361762.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chiari Type I Malformation in a Child with Syringomyelia and Scoliosis: A case report
- Two cases of Arnold-Chiari malformation type II
- A Case of Chiari Type 1 Malformation and Syringomyelia in Neurofibromatosis Type 1 Patient
- Treatment of Syringomyelia due to Chiari Type I Malformation with Syringo-Subarachnoid-Peritoneal Shunt
- A case of Arnold-Chiari malformation
